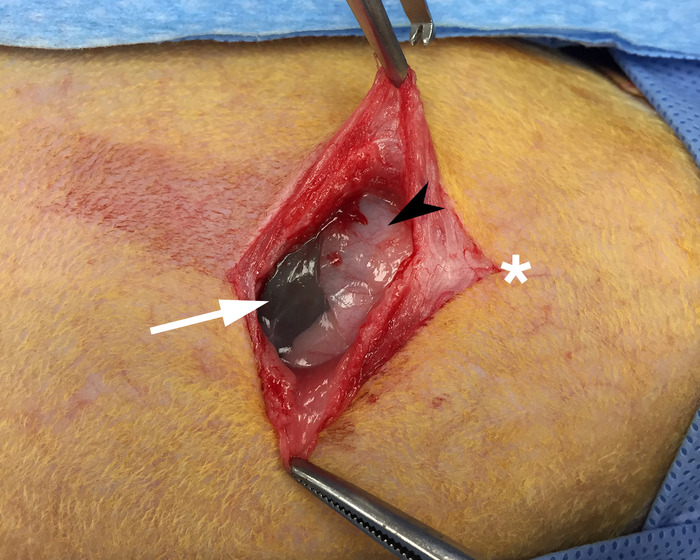
Figure 1: Exposed xiphoid process. Skin and underlying muscle have been reflected to allow for visualization of the xiphoid process (black arrow) and gut (white arrow). The white star denotes the cranial direction.
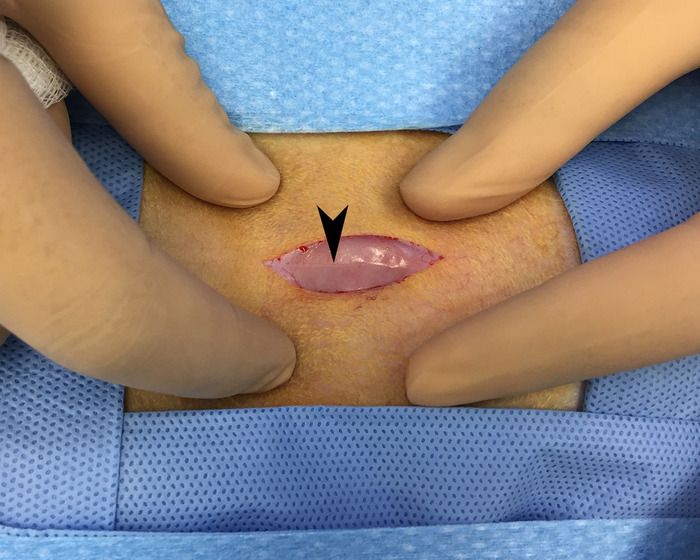
Figure 2: Linea alba. Overlying skin and fascia have been reflected to allow for visualization of the linea alba (black arrow) running in a cranial to caudal direction. This area is avascular and provides for blood-loss free access of the peritoneal space.

Figure 3: Lobe of liver outside peritoneum. This image shows a lobe of the liver that was gently extracted from the peritoneal space and placed on a piece of gauze.
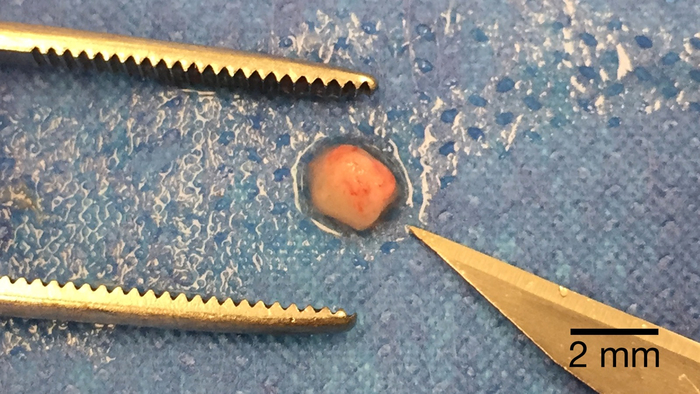
Figure 4: Post-processed tumor piece for implantation. A piece of tumor processed to the appropriate size for implantation placed next to the tip of a #11-blade for scale.
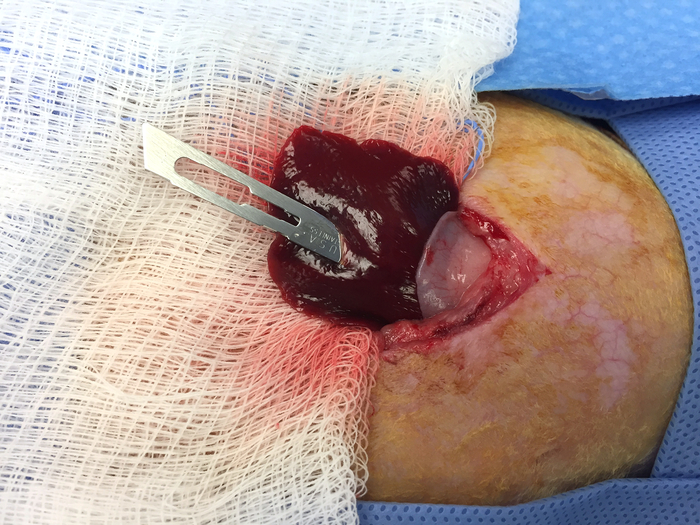
Figure 5: Creating a pocket in the liver for tumor implantation. An #11-blade is inserted to the appropriate depth in the extracted lobe of the liver. This will create an appropriately sized pocked for the implantation of the tumor piece from Figure 4.
