I. Preparation of Ovarian Tumor Cells
- Grow ovarian cancer cell lines expressing luciferase in culture. Sources of luciferase can be Firefly, Renilla, or other species. Cells expressing fluorescent proteins can also be used. For this demonstration we use an ovarian cancer cell line, OVCAR5, expressing firefly luciferase.
- Harvest cells using routine cell culture technique.
- Keep the cell suspension (10,000 cells/μL) in phosphate buffered saline (PBS) on ice until time of injection.
II. Intrabursal Injection
This procedure requires assistance from a second person. All surgical procedures are conducted under aseptic conditions. This includes wearing surgical attire and using sterile surgical instruments, syringe, and needles.
- Prepare the anesthetic solution by mixing 3 mL of ketamine hydrochloride (100 mg/mL), 1.6 mL of xylazine hydrochloride (100 mg/mL), 1.5 mL of acepromazine (10 mg/mL), and 20 mL of 0.9% sodium chloride.
- Check the animal’s identification number and observable health. Anesthetize the animal with prepared ketamine-xylazine-acepromazine anesthesia via intraperitoneal (i.p.) injection with a dose volume of 8~9 mL/kg body weight (BW).
- Confirm that the animal is under an acceptable plain of anesthesia by performing a toe pinch with forceps or fingers to the animal’s hind paws. If there is pedal reflex, wait for a deeper plain of anesthesia until the animal is unresponsive to this procedure.
- Lay the animal dorsal side up on a sterile gauze pad with its head facing away and its tail facing towards you. The point of incision is located to the left or right of the midline and above the ovaries. Shave or wet the fur with 70% alcohol at the incision point.
- Lift the wetted skin using forceps and make a small incision with the scissor at the dorsomedial position and directly above the ovarian fat pad. The ovarian fat pad should be visible beneath the surface of the peritoneal wall. Fat pad is easily recognizable by its white color in contrast to the dark pink tissue surrounding it.
- Gently lift the peritoneal wall lining and make a small incision as described above (5).
- Place a sterile soaked saline gauze pad on the midline adjacent to the incision. Locate the ovarian fat pad and gently pull it out and rest it onto the gauze. Stabilize the ovary by clamping the fat pad with a bulldog clip. Under a dissecting microscope, position the ovary as to allow for the insertion of the needle (30 gauge, G) into the oviduct tubule bend leading to the bursa. When the needle is inserted into the proper position, it should be visible under the bursa.
- Gently push the plunger of the syringe to inject 5 μL of cell suspension between the bursa and the ovary while the syringe is positioned to injection site. This step requires two people. One person pushes the plunger while the other person maintains positioning of needle. Remove the needle quickly to seal the puncture site but gently enough not to tear the bursa and tubule. The bursa should appear to be slightly distended with proper injection.
- Release the fat pad from the bulldog clip and gently replace the reproductive tract and fat pad back into the peritoneal cavity. Gently close the body wall by pulling the upper peritoneal lining over the lower lining. Close the skin with surgical staples or wound clips.
- Place the recovering animal back in its cage and provide a safe heat source to avoid hypothermia and speed up recovery. Monitor the breathing rate and ease, the return of muscle tone, and the ability to voluntarily move. These are all good indicators of the progression towards recovery. Staples or wound clips can be removed 7 or more days post surgery.
III. Oral Gavage Administration
- Use an 18~20 G gavage needle or feeding tube with a rounded tip. The gavage needle should be no longer than the distance from the tip of the animal’s head to its last rib.
- Check the animals’ identification number and observable health. Gently scruff the animal by grasping the skin over the shoulders with thumb and fingers. The restraint should be just firm enough for the fore limbs to be extended to each side and out of the way. The animal should not be able to grasp at the needle.
- Gently pull back the animal’s head with your index finger, forming a straight line through the neck and esophagus. Support the animal’s back with the inside of your thumb.
- Gently and without force, insert the gavage needle at either side of the mouth and over the tongue. In one smooth motion, the needle should pass against the roof of the mouth and down the esophagus. Gravity should guide the needle down without meeting resistance. If there is any resistance, remove the needle and start again. The animal’s gag and swallow reflex may be triggered during insertion. However, there should be no resistance or gasping from the animal. It is important to make sure that the animal is breathing when the needle is in place by checking the movement of the nostrils and chest.
- Slowly push plunger of the syringe to dispense the dose volume.
- Gently remove the gavage needle at the same angle and pathway as the way it was inserted down the esophagus.
- Return the animal to its cage and monitor breathing and behavior for 5~10 minutes.
IV. In Vivo Imaging
We use the Caliper Life Sciences to monitor the behavior of cells injected into intrabursal cavity. Experiments using this system typically have a timeframe of 4~16 weeks from the time of tumor implantation.
- Prepare the solution of D-luciferin (substrate of firefly luciferase) by dissolving 5~20 mg in 1 mL PBS and filtering through 0.22 μm membrane for sterilization.
- Charge the induction chamber by turning on both the oxygen and the isoflurane gas. Turn ON the gas flow to the induction chamber only. The isoflurane flow rate is maintained at a low level until animals are ready to be imaged.
- Check the animals’ identification number and observable health. Place the animal in the induction chamber charged with isoflurane gas.
- Remove the animal from the chamber when the animal appears to be anesthetized. Deliver 200 μL of prepared luciferin solution via i.p. injection using 30 G needle. It is important to record the time of injection in order to keep the time consistent between luciferin injection and imaging performance throughout the study.
- Place the luciferin-injected animal back into the induction chamber.
- Set the imaging system to the appropriate settings. Be sure to initialize the system before acquiring the first animal image.
- Turn OFF the gas flow to the induction chamber and turn ON the gas flow to the imaging chamber.
- Place the anesthetized animal dorsal or ventral side up. Be sure to place the animals’ nose in a nose cone to maintain proper anesthesia induction. Make sure the animal is within the “point of interest grid” as indicated by green illumination.
- Close the door of the chamber and acquire the image at the appropriate time. Time can be determined by kinetics.
- Remove the animal from the imaging chamber and place it back into its cage. Monitor the animals’ recovery as described in “Intrabursal Injection”.
V. Representative Results
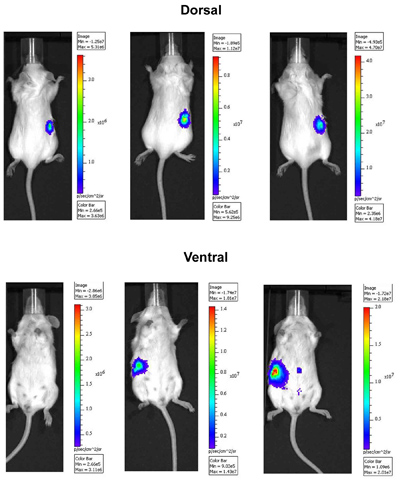
Figure 1. In Vivo imaging of ovarian tumor cells in an orthotopic mouse model. OVCAR5 cells expressing luciferase were injected intrabursally into right ovary and imaged over time. Images were taken 13 (left), 17 (middle), and 22 (right) days after the injection using the IVIS Spectrum imaging system. Dorsal side is shown in upper panel and ventral side is in lower panel. Note that the peritoneal spread of tumor cells 22 days following injection.
Experiments on animals were performed in accordance with the guidelines and regulations set forth by Fox Chase Cancer Center’s Institutional Animal Care and Use Committee.
