1. Pre-injection Preparations
- Fast the fish for at least 24 hours prior to injection. This will empty the intestinal bulb (stomach) contents. The basic fasting protocol is to transfer the fish, at their normal density, to a clean tank, then withhold food. For longer-term fasting that requires more rigorous conditions (e.g., for blood glucose studies), see additional considerations in the Discussion.
- Prepare Cortland salt solution (Perry et al., 1984).
For a 100 mL volume, dissolve the following in distilled water:
725 mg NaCl (124.1 mM)
38 mg KCl (5.1 mM)
41 mg Na2HPO4 (2.9 mM)
24 mg MgSO4∙7H2O (1.9 mM)
16 mg CaCl2∙2H2O (1.4 mM)
100 mg NaHCO3 (11.9 mM)
4 g Polyvinylpyrrolidone (PVP) (4%)
1,000 USP units Heparin
Filter, sterilize and store at 4°C. - Prepare the microscope.
- Cover the microscope base with plastic wrap for protection in case of spills.
- Put a paper towel on top of the plastic wrap. The surgical table will sit on top of the paper towel.
- Pre-adjust focus by viewing the surgical table and focusing on the sponge.
- Weigh the fish.
- Fill a 500 mL beaker about 1/3 full with fish facility water.
- Tare the balance.
- Collect the fish using a net. Wick excess water away from the net and fish by briefly dabbing the net on paper towels. Transfer the fish to the beaker.
- Weigh the fish.
- Transfer the fish to a clean tank.
- Transfer each weighed fish to its own labeled tank.
- Calculate the injection volume for each fish based on fish weight.
- Prepare the syringe and related injection equipment. For injection, we recommend a 35G beveled steel needle and a 10 μl NanoFil microsyringe. Prepare the NanoFil syringe and silflex tubing following the manufacturer’s instructions. It is important to remove any bubbles from the syringe and tubing. After filling the syringe and tubing, mount the syringe on the pump, and program the injection volume for the first fish.
- Prepare the surgical table.
- Cut a soft sponge (such as #L800-D, Jaece Industries) so that it is approximately 20 mm in height. On the flat face, make a cut that is 10-15 mm deep. This cut is the trough that will hold the fish for injection.
- Set the sponge into a 60 mm Petri dish.
- Set the Petri dish with sponge into a suitably-sized pipette tip box lid. The lid needs to be large enough to hold water to help maintain sponge temperature, but it should be shallow enough to not get in the way. We use a lid from a P200 tip box that is 11.4 cm L x 7.7 cm W x 1.5 cm D.
- Prepare the anesthetic.
- Make crushed ice using cubes made from fish facility water.
- Fill a clean ice bucket with the crushed ice.
- Put the surgical table into a larger container such as a 2.4 liter Rubbermaid food storage container.
- Pour some facility water (warm) into the outer container and the surgical table. Keep a reserve of warm facility water nearby.
- Put a thermometer into the outer container.
2. Anesthesia, Injection and Recovery
- Place the anesthetic outer container plus surgical table adjacent to the microscope. Have the bucket of ice chips nearby.
- Bring the water temperature down to 17°C by adding ice chips. Important: Don’t go below 17°C for this step.
- Use a net to transfer the fish to the outer container.
- Slowly add ice chips to the container to bring the temperature down to 12°C, over the course of several minutes.
- Monitor fish behavior: At 17°C or slightly lower, the fish typically will spread its pectoral fins horizontally, gasp, and have rapid operculum movements. As the temperature drops, the fish will swim more slowly and finally stop swimming. As the surgical plane of anesthesia is approached, gasping will stop and operculum movements will slow. The fish is ready for injection when it does not react to being handled. For most fish, 12°C is sufficient. Larger fish may require colder water.
- As the required temperature is reached (~12°C or colder), press on the sponge to saturate it.
- Keep your fingers in the cold water sufficiently so that they will not warm up the fish and bring it out of anesthesia during handling.
- With cold fingers, gently transfer the fish to the trough of the sponge. Position the fish with the abdomen up and the gills in the trough.
- Quickly transfer the surgical table to the microscope stage.
- Working quickly, carefully insert the needle into the midline between the pelvic fins. The needle should point cranially and be inserted closer to the pelvic girdle than to the anus. You should be able to feel when the needle is deep to the body wall. Inject the appropriate volume and withdraw the needle.
- After injection, immediately transfer the fish back to its warm-water (~28.5°C) tank for recovery by releasing the fish from the sponge over the tank water.
Tip: If the fish does not begin swimming immediately, help it to recover by gently swirling water towards the gills. - Check the needle. Occasionally a scale may be attached and should be removed prior to the next injection.
- For subsequent injections, use warm facility water to bring the anesthetic chamber water temperature back up to 17°C before introducing the next fish.
3. Representative Results:
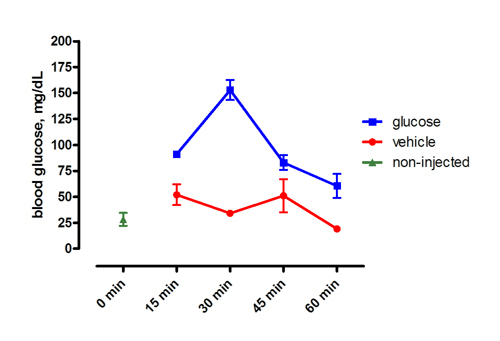
Figure 1. Representative results following intraperitoneal injection of 0.5 mg/g glucose or vehicle. Fish were fasted for 72 hours prior to injection. The x-axis shows time, post-injection. Mean ± SEM.
