1. DC nucleofection
- Harvest monocyte-derived DCs, which have been enriched using plastic adherence, cultured for 5 days using Cell Genix Media supplemented with IL4(1000U/ml), GMCSF (800IU/ml) and further matured for 24hrs using the DC maturation cytokines IL4(1000U/ml), GMCSF (800IU/ml), IL6100ng/ml, TNF-α 10ng/ml, IL1-β 10ng/ml and PGE2 (1μg/ml)1, by gentle resuspension with a 3ml transfer pipette.
- Count viable DCs using trypan blue, transfer into 3x 15ml tubes with no fewer than 0.5×106 and no more than 2×106 cells/tube.
- Centrifuge DCs for 10mins @ 200g. During this time pre-warm Cell Genix media supplemented with the DC maturation cytokines (DC maturation media) – 2ml/well in three wells of a 12-well tissue culture treated plate in a 37°C/5% CO2 incubator.
- Once cells have finished spinning, aspirate the supernatant and add the relevant DNA plasmids to each of the tubes in a final concentration of 5μg DNA/tube. In this case add the plasmid encoding IE1-pp65 to tube #1, Hexon-Penton to tube #2, and EBNA1-LMP2-BZLF1 to tube #3.
- Resuspend DCs and DNA with 100μl of Amaxa nucloefection solution, mix well and transfer to the nucleofection cuvettes.
- Place cuvettes in the 4D nucleofector, choose program CB150 (Amaxa/Lonza), and press start.
- Immediately after nucleofection add 500μl of the 2ml pre-warmed Cell Genix DC maturation media to the cuvette, mix gently by pipetting up and down 2-3 times, and transfer nucleofected DCs to the prepared 12-well plate containing the remaining 1.5 ml of prewarmed DC maturation media. Transfer to the 37°C/5% CO2 incubator for a further 12-18hrs.
2. T cell stimulation
- Harvest and count nucleofected DCs, and irradiate at 30Gy. Wash once with 10ml of CTL medium (45% RPMI, 45% Clicks EHAA, 10% FBS, 2mM Glutamax) and resuspend @ 3 x 105 DCs per ml of CTL media.
- Pool a minimum of 7.5×105 (2.5ml) and a maximum of 15×105 (5ml) of DCs containing each of the plasmids and transfer the pooled DCs to the G-Rex device which will then be placed in the incubator.
- For the preparation of responder cells use either previously frozen PBMCs or non-adherent mononuclear cells that remain after the DC selection (adherence or CD14 selection). Thaw the cells, transfer to prewarmed culture medium, wash once with CTL media. Resuspend the cells in CTL Media, count the cells and bring them to a concentration of 2×106 cells per ml. Take 15×106 cells or 7.5ml and supplement with 30000U IL4 (1000U/ml – final conc.) and 300ng IL7 (10ng/ml – final conc.).
- Transfer 7.5ml of PBMC (15×106 cells) to the G-Rex and top up the bioreactor with CTL media to a total volume of 30ml.
- Culture the G-Rex for 6-7 days in a 37°C/5% CO2 humidified incubator.
3. T cell expansion
- On day 6-7, aspirate 10ml of media, then mix the cells in the remaining 20ml of media with a 10ml pipette and count viable cells using trypan blue. If there are <50×106 replenish with fresh media + cytokines. If there are >50×106 cells remove 10ml of cell suspension, transfer to a new G-Rex, and then feed both G-Rexs with fresh CTL media + cytokines.
- Culture for an additional 4-6 days. Once sufficient cells have been expanded, perform phenotypic and functional characterization of the CTL and cryopreserve excess for future use.
4. Representative Results:
A schematic of our FDA-approved multivirus-specific CTL generation process is shown in Figure 1. In contrast to convention multivirus CTL protocols which use adenovectors and EBV-LCL to stimulate virus-reactive T cells2 we have replaced infectious virus material with DNA plasmids that encode multiple antigens derived from each of the viruses3. To stimulate trivirus CTL we designed three multicistronic plasmids encoding Hexon and Penton of adenovirus, IE1 and pp65 of CMV, and EBNA1, LMP2, and BZLF1 of EBV. These antigens were chosen based on encouraging clinical results of our own and other groups showing that T cells directed against Adv-hexon and penton2,4-6, and to CMV-1E1 and to CMV-pp65 are protective in vivo7. For EBV, EBNA1 is an immunodominant CD4+ T cell target antigen expressed in all EBV-associated malignancies and in normal EBV-infected B cells8,9, LMP2 is immunogenic across multiple HLA types and expressed in most EBV malignancies,10,11 while BZLF1 encodes an immunodominant, immediate early lytic cycle antigen that stimulates both CD4+ and CD8+ T cells from most individuals and is likely important for the control of cells replicating virus12. To further optimize our manufacturing methods we collaborated with Nature Technology who generated minimalized, antibiotic-free (FDA-compliant) plasmids for CTL stimulation13,14. Using this strategy we consistently achieve nucleofection efficiencies of >35% while maintaining high cell viability (data not shown)3. Figure 2 shows that the frequency of virus-specific T cells in response to optimized DNA plasmids as measured by IFNγ ELIspot, was greater than in response to conventional pShuttle-based expression plasmids expressing the same antigens (n=8 Adenovirus, n=4 CMV, and n=2 EBV). The optimal ratio of DC:PBMC was important for potent T cell stimulation as shown in Figure 3 where a ratio of 1:50 produced sub-optimal activation compared to a 1:20 S:R ratio (n=2 donors). Production of sufficient CTL numbers with broad antigen specificity is a pre-requisite for clinical efficacy against all three viruses. This is achieved by CTL culture in the G-Rex, which supports superior T cell expansion compared with conventional 24-well plates (Figure 4A)15, while the addition of IL4 and IL7 to cultures increases the repertoire and specificity as shown in Figure 4B where the frequency of T cells reactive against the CMV-pp65-derived HLA-A2 resticted NLV peptide was assessed in cultures generated in the presence or absence of IL4 and/or IL716,17. To assess the phenotype and functional capacity of the expanded cells we perform flow cytometric analysis, intracellular cytokine staining/IFNγ ELIspot, and Cr51 release assays on the final product for cryopreservation/infusion. Typically the generated cells are polyclonal with a mixed population of CD4+ and CD8+ T cells with antigen-specificity detectable in both T cell compartments. The CTL are able to kill viral antigen-expressing target cells but not virus negative partially-HLA matched targets, indicating that they should not induce graft-versus-host disease (GvHD) in vivo (Figure 5).

Figure 1. rCTL generation protocol. First, DCs are nucleofected with the viral antigen-encoding plasmids and then mixed with autologous PBMCs at an R:S of 10 or 20:1. Cells are expanded in the G-Rex for 10-14 days in the presence of IL4 and IL7, then harvested, counted, tested for function, identity and sterility, and then cryopreserved for clinical use.

Figure 2. Optimized DNA plasmids induce superior T cell activation in vitro. DCs were nucleofected with optimized, FDA-compliant plasmids encoding Hexon and Penton (Adv), IE1 and pp65 (CMV), and EBNA1, LMP2, and BZLF1 (EBV) or conventional pShuttle plasmids encoding the same antigens. These were used to stimulate T cells and specificity was analyzed by IFNγ ELIspot 10 days post-stimulation.
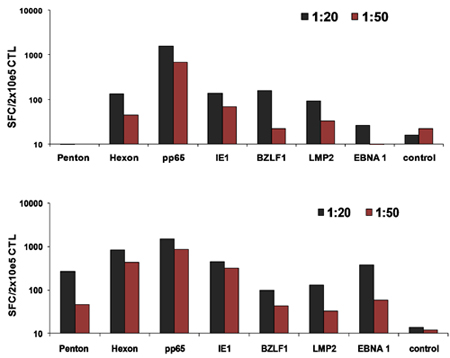
Figure 3. Optimal DC:T cell ratios for CTL activation. DCs from 2 donors were nucleofected with all three optimized plasmids and then used to stimulate autologous PBMCs at 1:20 or 1:50 DC:PBMC ratio. The frequency of reactivated T cells was assessed on day 10 by IFNγ ELIspot.
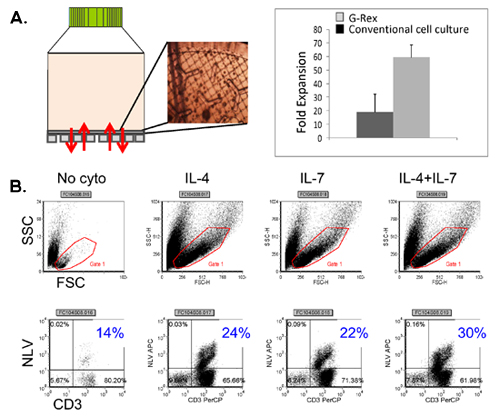
Figure 4. T cell expansion in the G-Rex using enhancing cytokines. Panel A shows the G-Rex device as well as CTL appearance on the gas permeable membrane, evaluated by microscopy. A comparison between cell output achieved in convention tissue culture treated plates vs G-Rex is also shown. Panel B shows the frequency of CMV pentamer positive CTL achieved in cultures expanded in the presence of no cytokine, IL4 alone, IL7 alone and IL4+IL7.
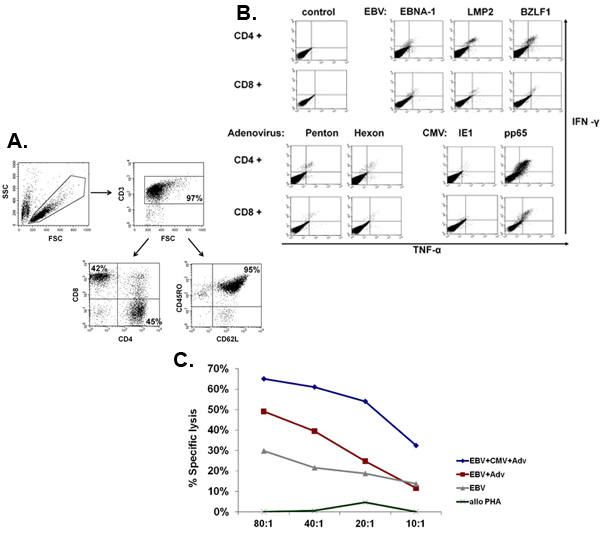
Figure 5. Phenotype and function of expanded CTL. Panel A shows a representative example of the phenotype of the expanded multivirus CTL, which are polyclonal with a mixture of CD4+ (45% – helper) and CD8+ (42% – cytotoxic) T cells, of which the majority (95%) expressed the memory marker CD45RO+/CD62L+. Panel B shows that these cells are specific for all the stimulating antigens and are polyfunctional as assessed by intracellular cytokine staining to detect production of IFNΓ and TNFα after antigen stimulation. Panel C shows that the expanded CTL are functional as measured by Cr51 assay. Autologous LCL, either alone or transduced with a null vector or an adenoviral vector expressing CMV-pp65 were used as targets. Alloreactivity was assessed using allogeneic PHA blasts as a target.
