1. Preparation of Hanks’ Balance Salt Solution (HBSS)
- Autoclave 1 L glass beaker, 1000 mL graduated cylinder, and stir bar.
- Reconstitute the HBSS powder solution in the autoclaved 1 L glass beaker to the 900 mL mark with double distilled water.
- Mix HBSS solution with 3.4 g of Hepes Na+ salt and adjust the pH to a value between 7.35-7.41 using either concentrated HCL or NaOH.
- Once the desired pH has been attained and remains stable, add 5 g of bovine serum albumin to the solution at room temperature until the albumin is completely dissolved.
- Add 10 mL of the antibiotic, antimyotic, to the solution and double distilled water until the total volume is at 1000 mL mark.
- Stir the solution thoroughly.
- Filter the HBSS solution and separate it into 50 mL Falcon tubes for later use. Additional tubes can be frozen and used at a later date.
2. Animal Preparation – Insertion of Tracheal Tube
- Prepare a tray with required instruments and material for insertion of a tracheal tube (i.e. forceps, scissors, tracheal tube, 3-0 black braided suture, small animal ventilator, etc.).
- Once the rat is completely anesthetized with a ketamine/xylazine cocktail in the ratio of 2 ketamine to 1 xylazine, shave the abdomen, chest, and throat of the rat. To ensure that a deep anesthetic state has been achieved, pinch the rat’s toe and check for pedal withdrawal of limb. Make sure the rat is deeply anesthetized before making all incisions.
- Place the rat with its head raised on a cutting board that is inclined at a 30° angle
- Make a skin incision from the mid-abdomen to below the lower jaw. Dissect away the muscles of the anterior triangle of the neck to expose the trachea.
- Place a 3-0 black braided suture under the trachea.
- Make an incision in the trachea between the cartilaginous rings and insert the tracheal tube. Tie the suture tightly to secure the tracheal tube to the trachea.
- Connect the tracheal tube to a small animal ventilator.
3. Instrument Preparation for Immune Cell Isolation
- Prepare a tray with the instruments for the immune cell isolation procedure (i.e. forceps, scissors, HBSS, trimmed soft Teflon 24 gauge Baxter intravascular over the needle quick-cath)
- Prepare two 10cc syringes, fill one syringe with HBSS for introducing the buffer into the pericardial sac and reserve the other one for aspirating the HBSS containing cells.
3.2.1. Reduce the Teflon tip of the 24 gauge Baxter intravascular over the needle quick-cath (1.6 cm) by 1/2 to 3/4 of its original length for the isolation procedure. - Place all syringes, buffers, and an empty 15 mL Falcon Tube (to hold the extracted fluid once procedure is finished) on ice.
4. Immune Cell Isolation
- Make a midline incision in the abdominal wall (along the linea alba) until you reach the xiphoid process.
- Starting slightly laterally to the xiphoid process, make bilateral incisions through the rib cage continuing at an angle toward the axilla. Be careful not to perforate the lungs, heart, or pericardium.
- Once the incisions on both sides of the sternum are complete, dissect away the diaphragm from the lower ribs, cutting lateral to medial.
Note: Be ever aware of where the pericardium connects to the diaphragm and sternum to avoid damage. Use the falciform ligament as a landmark to note where the pericardium is attached on the opposite side of the diaphragm. Also, if the pericardium is cut, the ability to isolate cells is lost. - Gently lift one side of the ribcage to expose the thoracic cavity and the heart (still encapsulated by the pericardium).
- Take the HBSS filled syringe and find a point in the pericardial sac approximately half way between the sternum and the heart (preferably more rostral than caudal) and insert the Teflon tip of the shortened quick-cath through both layers of the pericardium.
- Once the catheter is in place, proceed gently fill the pericardial space with 2 to 3 ml of HBBS buffer. You will know immediately if the catheter is properly placed when you notice the pericardial space expanding. If no filling is witnessed, withdraw and reposition the quick-cath.
- When the pericardial sac is filled, take the other 10 cc syringe and place the tip back in the pericardium and begin aspirating the buffer. The same entry hole can be used or another can be created. Make sure the tip does not come too close to the walls of the pericardial sac while providing suction, especially on the underside of the heart. This could lead to puncturing the pericardial sac and loss of cell-containing cells.
- While aspirating the buffer, the catheter tip can be moved around inside the pericardial sac in order to collect as much buffer as possible.
Note: If in doing so you slightly tear the pericardium and make the hole at the top of the heart larger than the original hole, don’t panic. As long as the pericardium still surrounds enough of the heart you can still perform another wash over the heart albeit with a lesser amount of buffer. For collection of an optimal amount of cells, three to four additional washes are needed.
- Place the extracted buffer into the Falcon tubes that were placed on ice.
- Remove heart, lungs, and/or any other tissue if needed for further studies. After the collection of immune cells and other tissues, the rat must be rapidly and humanely euthanized.
- Centrifuge the collected immune cell samples for 10 min at 200g at 4°C. Always keep the tubes on ice when not in use.
- Remove the supernatant and reconstitute the pellet in 1 mL of Hyclone Buffer or HBSS.
Note: It is important to count the number of immune cells obtained from each heart after the immune cell isolation procedure.
5. Representative Results:
An example of isolated cardiac mast cells obtained with this technique and stained with toluidine blue and safranin O/ alcian blue are presented in figures 2A and 2B, respectively. As can be seen in Figure 3, The cardiac mast, maintained their ability to release histamine after treatment with known activators such as compound 48/80 and substance P as described in Morgan et al.9Representative scatter plots from flow cytometry of CD4+ cells and CD8+ cells are presented in figures 4 and 5, respectively. T-lymphocytes are further identified and phenotyped as a cell population from this technique.
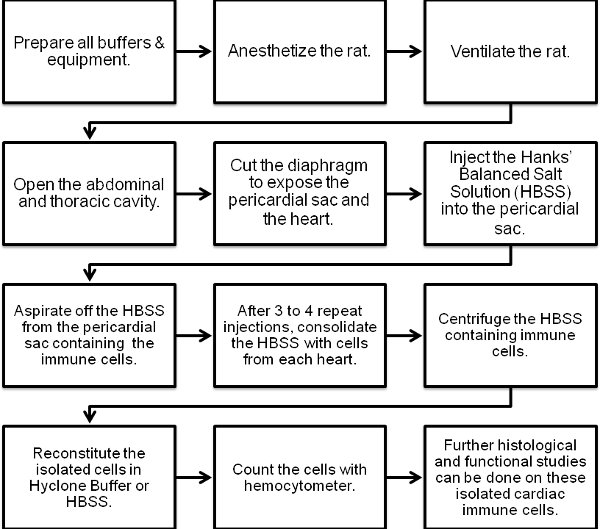
Figure 1. Flow chart of the cardiac immune cell isolation procedure.
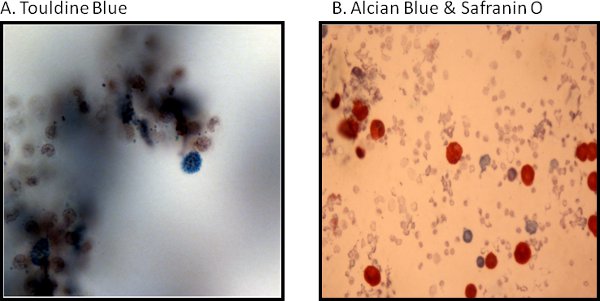
Figure 2. Histological representative images of cardiac mast cells are stained as follows: (A) with toluidine blue and (B) are safranin O/alcian blue.
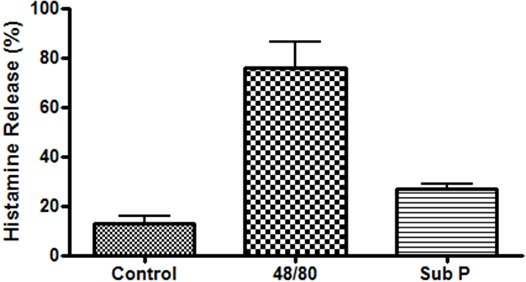
Figure 3. Functional study of cardiac mast cells isolated from the epicardial myocardial region and stimulated with compound 48/80 (10μg/mL) and substance P (10μM).
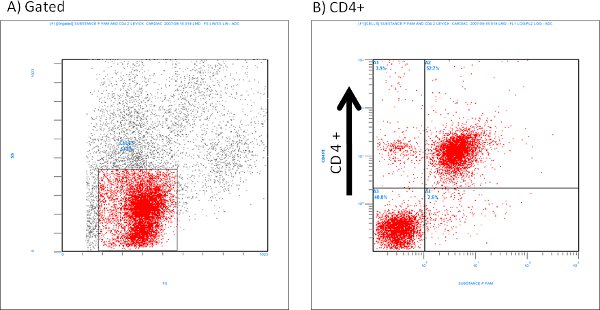
Figure 4. Representative flow cytometry scatter plots of isolated CD4+ cells labeled with Substance P (1:100 dilution).
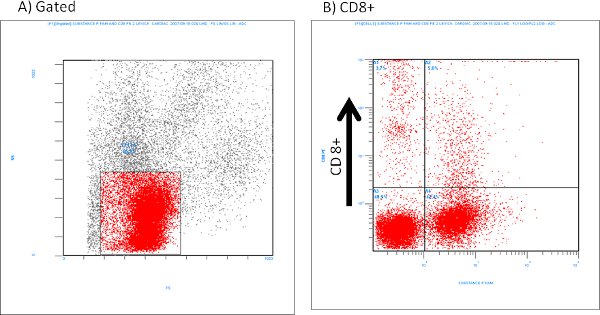
Figure 5. Representative flow cytometry of isolated CD8+ cells labeled with Substance P (1:100 dilution).
