After creating a thinned window over the cerebral cortex the vasculature should now be more visually prominent (Figure 1) and will allow for a deeper imaging depth (up to 1 mm). The right cortex is thinned to approximately 55 μm as compared to a normal skull measured at 140 μm (Figure 1) and provides greater optical clarity. Further thinning to 10-15 μm is possible11 however not necessary as the use of glass cover slips and skull plates are not implemented in our experiments (Figure 1 and 2). This particular method has allowed us to identify specific structures (cerebral cortex, corpus callosum) in our OCT cross-sectional images (Figure 3). Parasagittal OCT images of a normal skull (Figure 3A) versus a thinned skull (Figure 3B) are shown to compare the outcome of an OCT image with a successful TSCW. Additionally, a coronal cross-sectional OCT image is also obtained to facilitate in identifying midline structures (Figure 3C). The maximum signal intensity for Figure 3 is 45 dB above the noise floor. An intensity profile comparison of a non-thinned skull and a thinned skull reveals a greater signal intensity and depth penetration in a TSCW model (Figure 4).
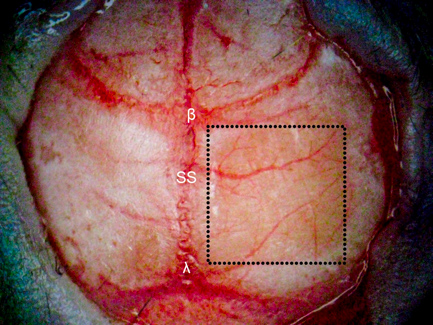
Figure 1. TSCW in a mouse model. A 4 × 4 mm thinned skull window (denoted in the dotted square box) is created ~ 1 mm posterior and lateral to bregma over the right cerebral hemisphere using various dental burs. The right cortex (thinned to approximately 55 μm) is significantly more transparent than the non-thinned skull (left cortex, 140 μm) providing greater depth penetration for optical imaging using OCT. β = bregma, λ = lambda, SS = sagittal suture.

Figure 2. OCT imaging of TSCW in vivo. A mouse model with a thinned-skull is fixed in a stereotactic frame under the objective for OCT imaging in vivo.
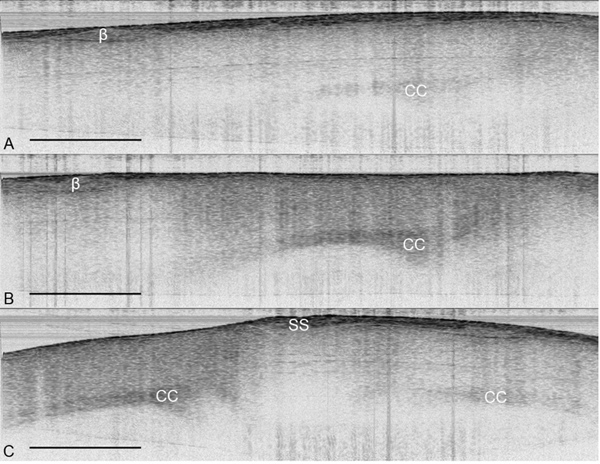
Figure 3. OCT images of the cerebral cortex in vivo. (A) Parasagittal OCT image of the cortex under a normal skull. (B) Parasagittal OCT image of the cortex under a thinned skull. (C) Coronal OCT image of a thinned skull (left) and a normal skull (right). The structures of the brain are more visually apparent under a TSCW as compared to a normal skull. OCT images from were obtained from the same mouse in vivo with imaging size 5.5 mm × 2 mm with maximum signal intensity of 45 dB. β = bregma, CC = corpus callosum, SS = sagittal suture, scale bar = 1 mm.
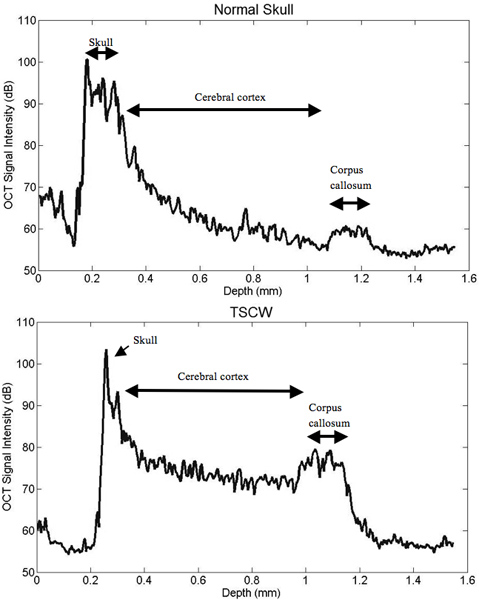
Figure 4. Intensity profile comparisons of normal and thinned skull prep. TSCW permits increased signal intensity and depth penetration. The TSCW achieves an imaging depth of about 1 mm with sufficient SNR.
