Multiple studies have characterized differences in gene expression, DNA methylation and cell subset in blood among individuals with and without mental (or other) illnesses1-4. These studies, however, have been obtained from clinical settings in which disease-associated differences may be magnified due to the generally more severe nature of the illnesses for which patients are seeking treatment. Due to advances in “omics” approaches, the past decade has seen an explosion of interest in obtaining biologic samples from community and/or epidemiologic settings5-7, in order to provide population-based estimates of disease prevalence and a broader picture of the environmental determinants of these mental and/or physical illnesses.
A key challenge in this regard is the requirement for rapid processing of the collected specimens. Degradation of mononuclear cells, key immune system components that are frequently used to assess the health of an individual, begins immediately upon blood draw with a significant decrease in recovery after 2 hr of collection8-10. To address this challenge, we present an optimized protocol in which multiple components of human whole blood are simultaneously isolated from samples obtained in homes of subjects living in a large metropolitan area. The protocol is based upon our compilation and modification of current techniques, including storage of all “extra” fractions in the event future techniques allow for further isolation/analyses. While alternative methods or kits may be employed in place of the individual methods described here, those outlined have proven to be a reliable and efficient means for processing samples in a high-throughput manner. High-quality fractions (PBMCs, DNA, serum, and RNA) of fresh blood can be produced within 2 hr of collection and all assay-ready specimens can be available within 2 days (Figure 1).
This protocol was developed to enable the efficient processing of samples collected from community-dwelling, adult residents of the city of Detroit for testing in the Detroit Neighborhood Health Study (DNHS; DA022720, RC1MH088283, DA022720-05-S1), a population-based study of the social and biological determinants of post-traumatic stress disorder (PTSD) and other mental illnesses. The prevalence of PTSD in Detroit is more than twice the national average11,12. Identifying biological determinants of PTSD in this population may help to develop appropriate pharmacologic and/or cognitive-behavioral interventions to aid those suffering from the disorder, both in this urban population, and in other high-risk populations (e.g., returning military veterans). Our laboratory, previously located at Wayne State University in Detroit, Michigan, was selected for processing based on our expertise in handling fresh tissue samples derived from a variety of sources, the necessity to begin processing the samples within 2 hr of collection, and our proximity to the collection sites. With this unique opportunity at hand, our goal was to optimize the processing for greatest yield of DNA, RNA, serum and peripheral blood mononuclear cells (PBMCs) from each specimen (a total of N=1,639 samples over 5 waves of specimen collection). The procedures outlined here can be performed simultaneously in a non-clinical setting, thus producing starting material (see Table 1 for average yields) for a multitude of downstream applications including microarray, epigenetic, real-time RT-PCR, and flow cytometry analyses.

Figure 1. Overall work flow. The overall process depicted here includes the logistics of obtaining the blood specimens from identifying consenting participants to the blood draw itself. High-quality, fractions (peripheral blood mononuclear cells; PBMCs, DNA, serum, and RNA) of fresh whole blood can be produced within 2 hr of collection and all assay-ready specimens can be available within 2 days. Moreover, the fractions prepared through this method are suitable for long-term storage if samples are not to be tested immediately. The entire timeline outlined here could be completed in a single day (~5 hr total). However, such a day would be extremely labor intensive especially for a single technician with substantial experience with the techniques. Thus, we recommend dividing the procedures on Day 1 between at least two technicians and completing the RNA processing on Day 2. Please click here to view a larger version of this figure.
It is essential that the overall procedure produce high quality material for analysis in a multitude of downstream applications including gene expression via microarray and RT-PCR analysis, detection of epigenetic modifications, and cell subset variations. Table 1 indicates the average yield and quality of materials from each of the processes. Figure 3 provides an example of the quality output of the leukocyte RNA isolation and filter processing methods. The image on the upper left of Figure 3 is the gel image resulting from the capillary electrophoresis. Each lane should produce two distinct bands with minimal shadowing which would indicate degradation. The chromatograms below the gel provide an additional look at the level and type of degradation that can be determined based upon the location and size of the peaks. The RNA Integrity Number (RIN) is another quality measure that ranges from 1 (low; degraded) to 10 (high; pure, good quality RNA).
Such a high-throughput methodology lends itself to an occasional error, but there are several checkpoints throughout the various stages of processing to ensure quality control. Figure 2 displays the proper separation following centrifugation of the Ficoll containing vacutainer. There are several reasons a vacutainer may not display this separation including an error in centrifugation speed, low collection volume, or lack of a fasting participant as indicated in Table 2.
Subsets (n=100) of the specimens isolated using this procedure have been analyzed with success by HumanMethylation27 (HM27) DNA Analysis BeadChips including validation of those results by pyrosequencing11. Genotyping, targeted bisulfite pyrosequencing, and real-time RT-PCR has been successfully performed in the Wildman and Uddin laboratories20,21,22,23. Serum, isolated in parallel with the DNA isolation for both the Beadchip and genotyping analyses, was successfully analyzed for IL-6 and C-reactive protein activity24. T-cell subsets from the isolated PBMCs have been successfully analyzed by flow cytometry25-28. Additionally, RNA from the modified leukocyte procedure has been subjected to Genome Wide gene expression profiling 29.
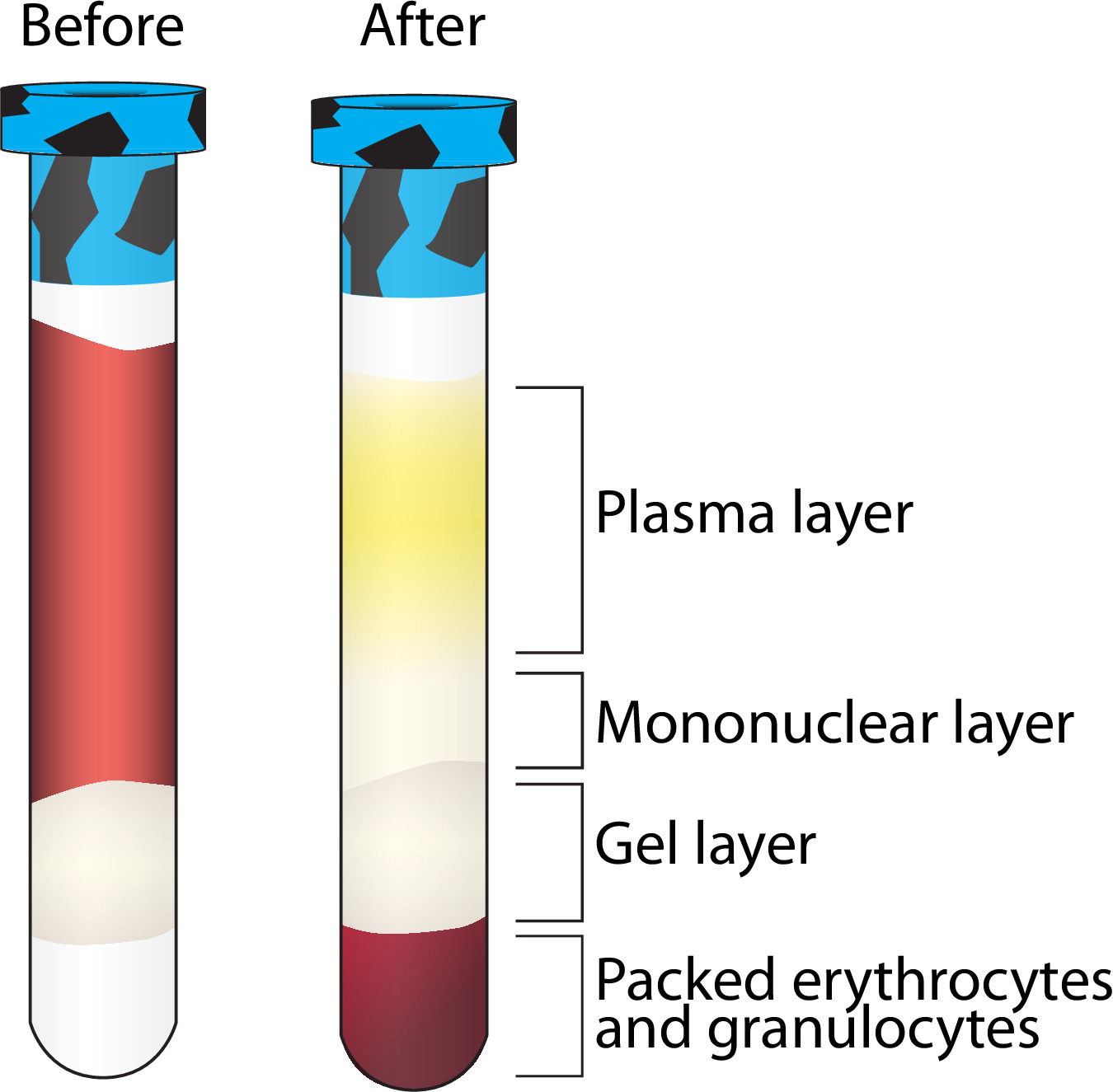
Figure 2. Layer separation following centrifugation of Ficoll containing vacutainer. A visualization of the separation of multiple blood components following centrifugation. The mononuclear layer is further purified while the other layers are stored at -80 °C. Please click here to view a larger version of this figure.

Figure 3. Expected results from leukocyte RNA processing. Bioanalyzer results displaying two distinct bands representing 18S and 28S ribosomal RNA with RNA integrity numbers (RINs) above 8 isolated with the described leukocyte RNA isolation and filter processing methods (see protocol 3.6 and 5.3). Please click here to view a larger version of this figure.
| Total Average Yield (N≈500) | Average Quality | |
| Serum | 2.30 ml | N/A |
| DNA from whole blood | 39.97 µg | Absorbance at 260/280 = 1.74 |
| PBMC | 22.25 million viable cells | At least 95% viability of overall isolation |
| RNA from Leukocytes | 44.09 µg | Absorbance at 260/280 = 2.01 RNA Integrity Number (RIN) = 6.48 |
Table 1. Expected yields. Average quantity and quality of samples processed using the described methods.
| Problem | Potential Solution |
| No separation after Ficoll containing vacutainer centrifugation | Vacutainer is not filled to capacity — the minimum collection volume for adequate processing is 6 ml. |
| Check centrifuge settings, be sure the speed is in g-force. If incorrect, set to g-force and respin. | |
| Low PBMC count | Volume of blood draw too low. |
| Aspirated too close to the pellet in step 3.7.8 | |
| Non-fasting participant. | |
| No separation after serum vacutainer centrifugation | Check centrifuge settings, be sure the speed is in g-force. If incorrect, set to g-force and respin. |
| Unexpected concentration using the Nanodrop 1000 | Make sure the measurement is for the appropriate sample type (e.g., DNA or RNA). |
Table 2. Troubleshooting. Common problems encountered with the described methods and potential solutions.

Supplementary Table 1. Tracking sheet. An example of tracking the vacutainers from blood collection to laboratory delivery. Please click here to view this table.

Supplementary Table 2. Specimen log. An example of the document used to document the processing of the vacutainers upon delivery to the lab. Please click here to view this table.

Supplementary Table 3. Cryovial Numbering System. An example of the numbering system used for each participant. Please click here to view this table.
Supplementary Information 1. Preprocessing details. Details the duties of the Study Coordinator, Courier and Phlebotomist. Please click here to view supplementary information 1.
Supplementary Information 2. Recipes. A list of recipes for the necessary reagents. Please click here to view supplementary information 2.
