Proper procedures to minimize motion artifacts result in high-quality diffusion weighted images of the rat cervical spinal cord. Using custom respiratory gating (Figure 2), saturating unwanted signal from tissues outside the spine (Figures 3B & C), and magnetic field susceptibility distortion correction produces diffusion-weighted images such as those in Figures 4 and 5. Improper or un-gated images will lead to artifacts in the form of ghosting (Figure 3E), whereas correct gating is free of artifacts.
Visual inspection of the diffusion weighted images across the 12 slices reveals features of the spinal cord that relates to its microstructure. Specifically, faster diffusion in the tissue results in greater signal loss on diffusion weighted images, which is exacerbated with greater diffusion weighting (b-value). With diffusion weighting performed perpendicular to the spinal cord axis, white matter along the periphery of the cord appears bright, since the diffusion is slow and restricted perpendicular to the axons. In contrast, the gray matter within the central region of the cord appears darker, since it is composed of axons and cell bodies that are not all aligned along a single direction. In comparison, diffusion weighting in the parallel direction results in white matter with a darker appearance, since diffusion is fast along the axons, whereas gray matter is relatively brighter. It is important to note that the separate diffusion weighted images are shown for different b-values, since the parallel and perpendicular directions have the best contrast between white and gray matter at different b-values.
Combining all of the diffusion weighted images using mathematical formalisms allows maps of the diffusion parameters to be shown. The average signals from the white and gray matter are plotted against the diffusion weighting factor (b-value) for the parallel and perpendicular directions. This quantitative data reinforces the diffusion weighted images shown in Figure 4. Specifically, white matter has a strong dependence on the direction of the diffusion weighting (longitudinal or transverse), whereas gray matter is less dependent on the direction. Similarly, fitting of the signal at each voxel using the equation for diffusion kurtosis yields quantitative maps of diffusion parameters (Figure 6B), which highlight this same dependence. White matter has a high degree of anisotropy for both the diffusion (AID) and kurtosis measurements (AIK). Thus, transverse diffusion and kurtosis reveal the underlying microstructure of the spinal cord that is known from histological studies. These diffusion parameters, which are acquired in live, but anesthetized animals, reflect microscopic tissue properties such as axon density and diameter. Alterations in these measures caused by injury and disease will be useful for noninvasively evaluating the consequences of injury and the effects of promising therapies. Diffusion weighted imaging of the rat cervical spinal cord may therefore become a tool for preclinical studies of spinal cord injury and diseases of the spinal cord.
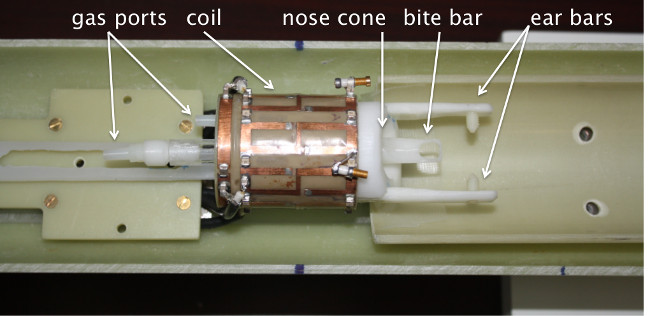
Figure 1: Design of the coil and holder for cervical spinal cord MRI. A custom quadrature volume coil (Doty Scientific Inc) was used to image the cervical spine with high sensitivity and uniformity. Anesthesia and medical air are delivered by the indicated gas ports into the nose cone, which fits comfortably around the nose of the rat. Exhaled and excess gas is captured by the exhaust line under slight vacuum. The head of the rat is secured with the bite bar placed around the incisors and the ear bars placed delicately within the ear canal. Other physiologic monitoring components, including the respiratory monitor and temperature probe are not shown.
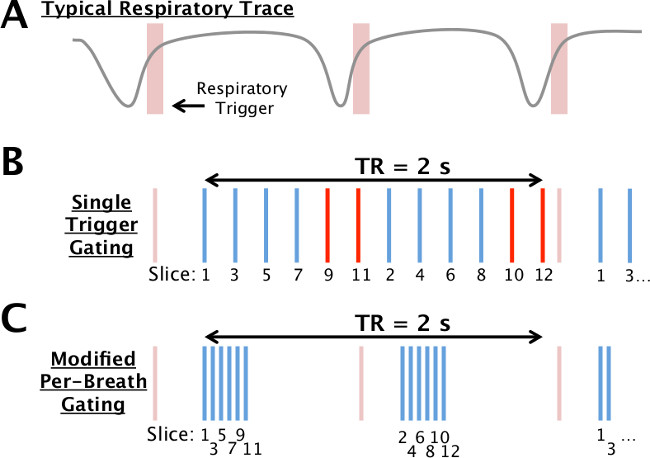
Figure 2: Respiratory gating scheme. A typical respiratory trace (gray) and trigger (red) from the gating unit are shown schematically (A). In the typical implementation of gating (B), a single trigger is used to acquire all slices (vertical lines; 12 shown here) at times evenly-spaced within the repetition time (TR). If the TR exceeds the typical period, several slices may occur during a breath and be susceptible to motion (red). In the modified scheme (C), a subset of slices are acquired rapidly after the trigger (6 shown here) followed by a delay, with the other slices acquired after the subsequent trigger. Effectively, the TR is identical between the two schemes by rearranging the delays within the sequence.
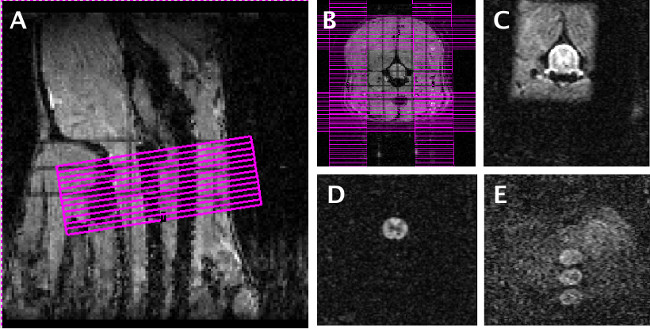
Figure 3: MRI slice positioning, saturation bands, and motion control. Twelve axial slices were arranged on the scout image (A) with the most anterior slice positioned at a consistent distance from the intersection of the brainstem and cerebellum. Saturation bands (B) were added to eliminate unwanted signal outside the area of interest. An image without diffusion weighting (C) and one with diffusion weighting (D) with the custom gating scheme employed clearly show the anatomy of the cord and is free of artifacts. With the non-optimized gating scheme or improper respiratory gating, diffusion weighted images show artifacts (E) as a loss of signal within the cord, or multiple “ghosts” outside the cord that will corrupt subsequent analysis. Please click here to view a larger version of this figure.
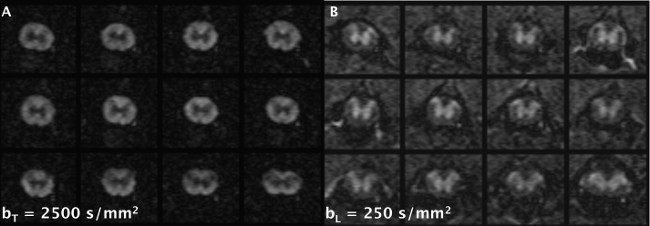
Figure 4: Representative diffusion weighted images. Using the optimizations described in the text, high-quality diffusion weighted images were obtained with diffusion weighting applied transverse (A) and longitudinal (B) to the spinal cord main axis. Different b-values are shown for each direction that provide the best contrast between the white and gray matter for illustrative purposes. For each direction or b-value, all 12 slices were acquired in approximately 90 sec. Please click here to view a larger version of this figure.
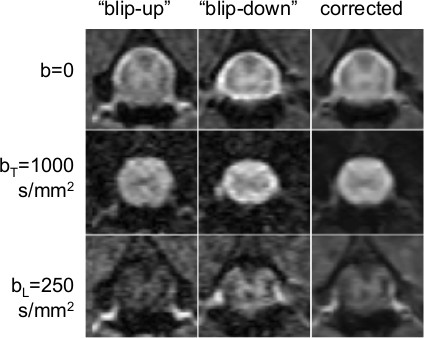
Figure 5: Reversed phase-encode correction process. The left column shows a single slice imaged with the DWI sequence as outlined in this protocol (“blip up” image). The middle column shows the sequence acquired a second time with the “reverse blips” set to ‘on.’ Note how features that appear stretched in the first image appear compressed in the middle column. The right column shows the diffusion weighted images corrected using TOPUP. The top row is the non-diffusion weighted image, the middle row is an example with diffusion weighting applied in the transverse direction, and the bottom row is an example with diffusion weighting applied in the longitudinal direction. Please click here to view a larger version of this figure.
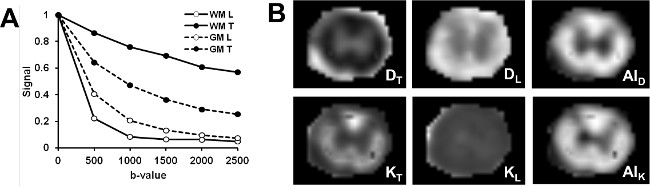
Figure 6: Computed maps of diffusivity and kurtosis. The normalized signal (image intensity) is plotted (A) as a function of diffusion weighting (b-value) for the transverse (T) and longitudinal (L) diffusion encoding direction. High-quality maps (B) of diffusivity (D), kurtosis (K), and anisotropy (AI) are calculated from the signal at each voxel and reveal unique features of the spinal cord tissue. Specifically, there is clear difference in parameters between the white and gray matter, as well as regional differences in the white matter regions. Please click here to view a larger version of this figure.
