Typical results obtained from the oscillatory rheological measurements on both the solution and the gel are shown in Figure 1. For injection through a long catheter, a Newtonian fluid with low viscosity is desirable. Viscosity was measured as function of shear rate, showing that at pH 8.5 the solution is shear thinning but at pH 9.0 and 9.5 the solutions behave as Newtonian fluids as evidenced by the constant viscosity of 0.54 and 0.36 Pa·sec, respectively (Figure 1A). After neutralizing the samples, the samples show a solid-like response observed by a storage modulus G′ which is larger than the loss modulus G″ and therefore a tanδ = G″/G′ <1 (Figure 1B). The gel obtains its final strength within 30 minutes. Oscillatory rheological measurements show a typical solid-like response with G′ almost independent of the angular frequency and G′ >G″ for all frequencies measured (Figure 1C).
Essential for the use as drug delivery system is the erosion of the hydrogel over time. The supramolecular interactions are inherently dynamic and allow for a slow erosion of the gel in vitro. Erosion and release experiments are performed at 37 °C using porous well inserts (Figure 2A and B). By tuning the length of the hydrophobic and hydrophilic block14, a gel that erodes over a period of several weeks can be obtained (Figure 3A). The gel erodes 25% in 2 weeks with an initial erosion of 10% in the first day, presumably due to initial swelling of the hydrogel. As example, both the release of a small molecule drug (pirfenidone), and the release of a model fluorescent protein (mRuby2) was studied. A fluorescent model protein allows for an easy readout; however, in vitro release experiments can also be performed on other proteins using ELISA for quantification6. The small molecule drug is released within a day, while bigger molecules such as proteins are gradually released over 1 week (Figure 3B). Fitting the release profile of mRuby2 up to 60% release with the semi-empirical Korsmeyer-Peppas model indicates release due to diffusion (n = 0.44)23. The absence of an offset in the (adapted) Korsmeyer-Peppas model shows that there is no burst release present for mRuby224. Because of the limited amount of data points with a release lower than 60% for pirfenidone, no fitting was performed on this release profile.
The catheter navigation system consists of a communication unit console, a workstation (Figure 4), a triangular location pad (generating a low magnetic field) with an external reference patch, and two catheters, the sensor-tipped mapping and the injection catheter (Figure 5).
After post-processing analysis has filtered unstable points the 3D endocardial reconstruction of the LV is updated in real time with the acquisition of each new data point and is continuously displayed as unipolar and bipolar voltage potentials on a graded color scale (Figure 6A). The local linear shortening (LLS) function quantifies regional wall motion by obtaining the average change in distance between sample site and adjacent points at end-systole and end-diastole. The mean voltage and LLS values are calculated for each segment and displayed in the polar map. (Figure 6B). The presence of an abnormal or low unipolar potential (≤6 mV) and impaired mechanical activity (LLS ≤4%) characterizes infarcted areas22.
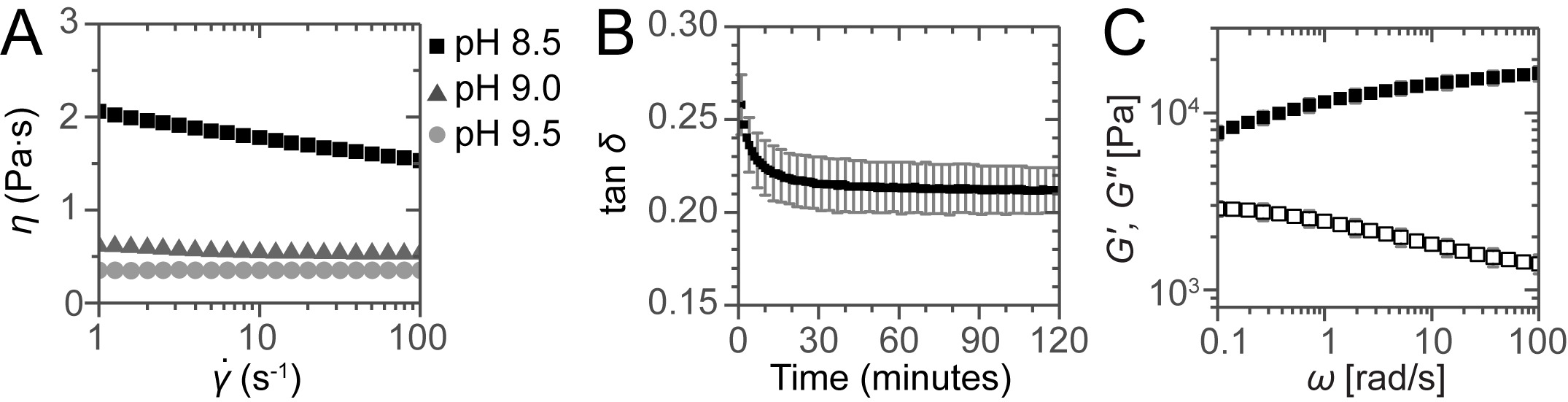
Figure 1:. Rheological assessment of the solutions and gels. (A) Viscosity as a function of shear rate for the solutions at different pH. For the sample at pH 8.5 shear thinning is observed but for the samples at pH 9.0 and 9.5 constant viscosities are obtained, showing the Newtonian behavior of these solutions. (B) Gel curing followed by plotting tan δ as a function of time. (C) Frequency sweep for a neutralized sample after 2 hr curing. Error bars show standard deviations of 3 independent measurements, indicating a typical experimental error.
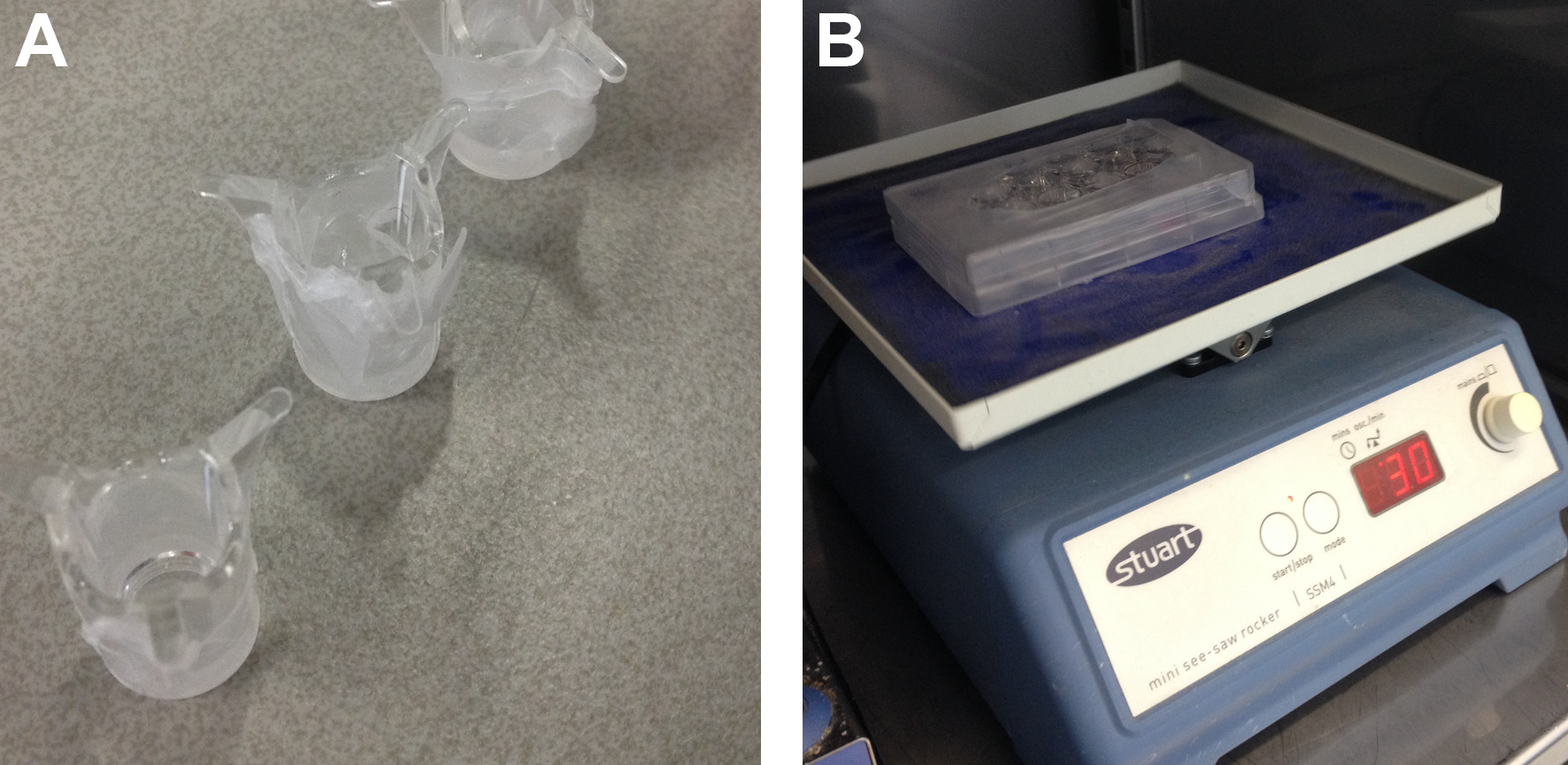
Figure 2: Setup for degradation and release experiments. (A) Poly(ethylene terephthalate) well insert covered with Parafilm to prevent leakage during preparation. (B) 24-wells plate with inserts, wrapped with Parafilm to prevent evaporation of the solvent.
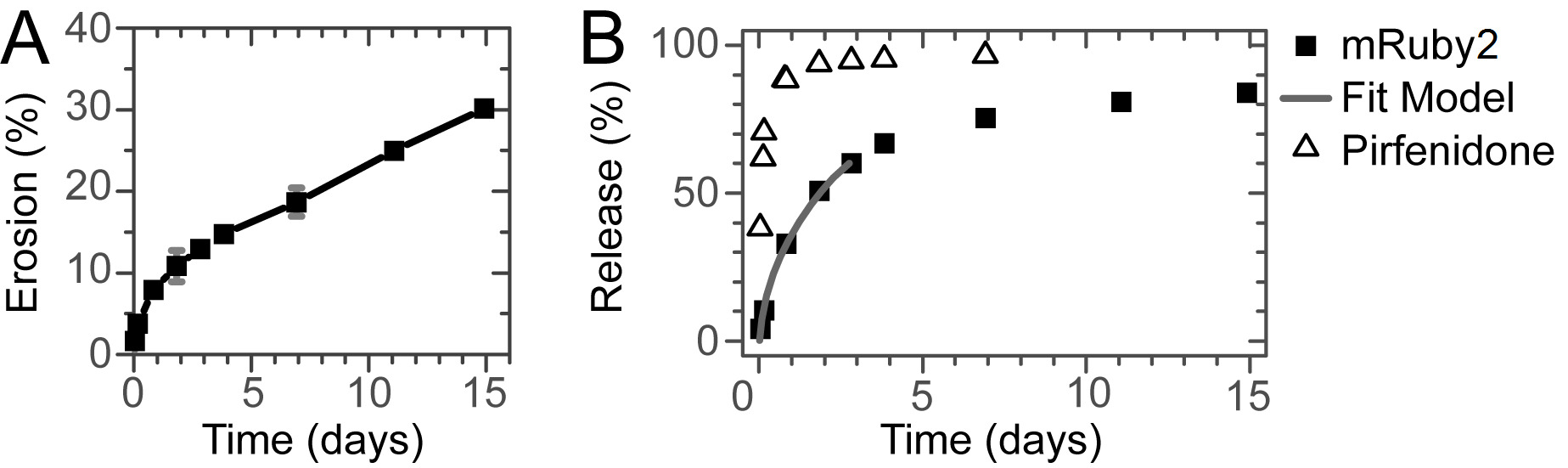
Figure 3: Erosion and Release. (A) Erosion of the hydrogel over time. Gradual erosion of the gel for at least 2 weeks is observed. (B) Release of a small molecule drug and a model protein. While the small molecule is released within a day, the model protein is gradually released over a week without a significant burst release. The line shows the fit of the Korsmeyer-Peppas model to the initial stage of the release.
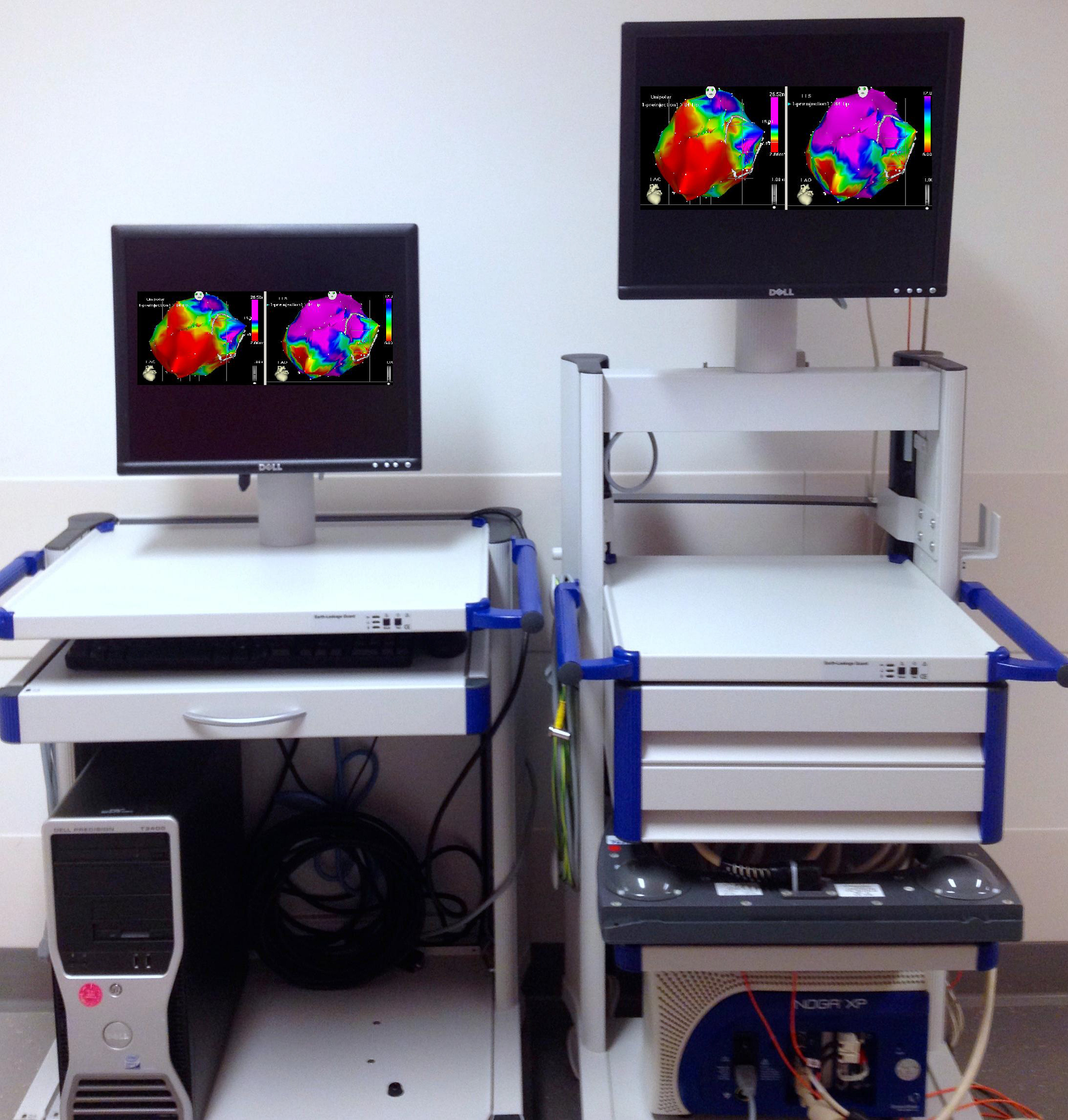
Figure 4: The catheter navigation system. Communication unit console with NOGA XP Cardiac Navigation System.
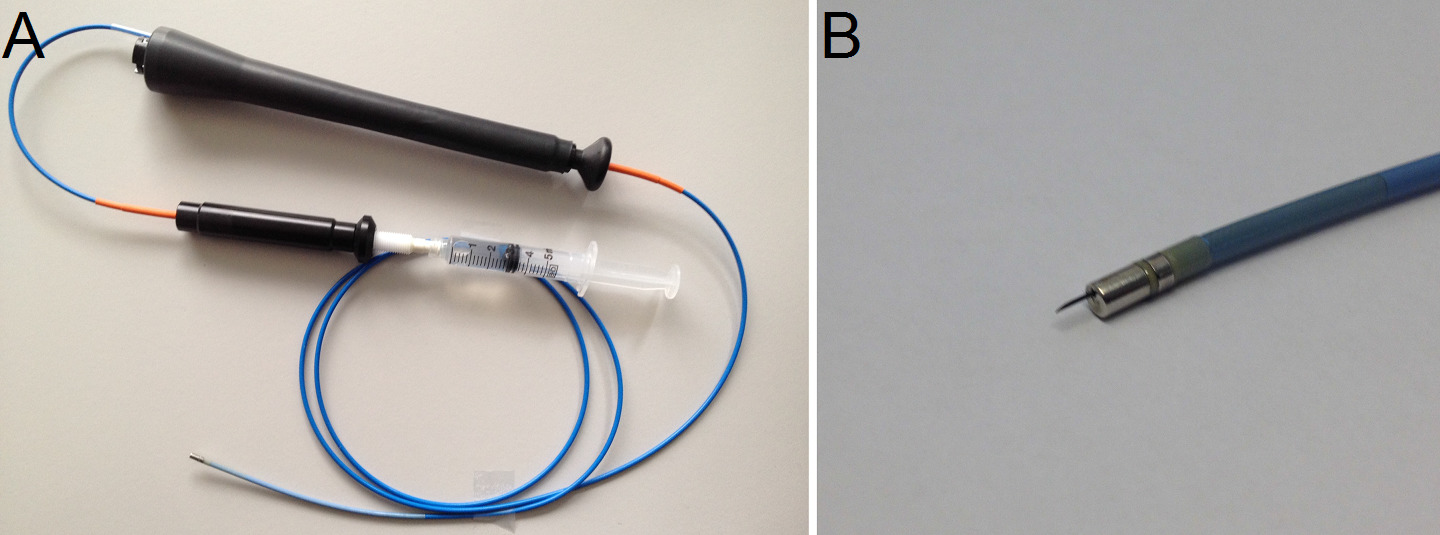
Figure 5: (A) The intramyocardial injection catheter with syringe attached. (B) Detail of injection needle.
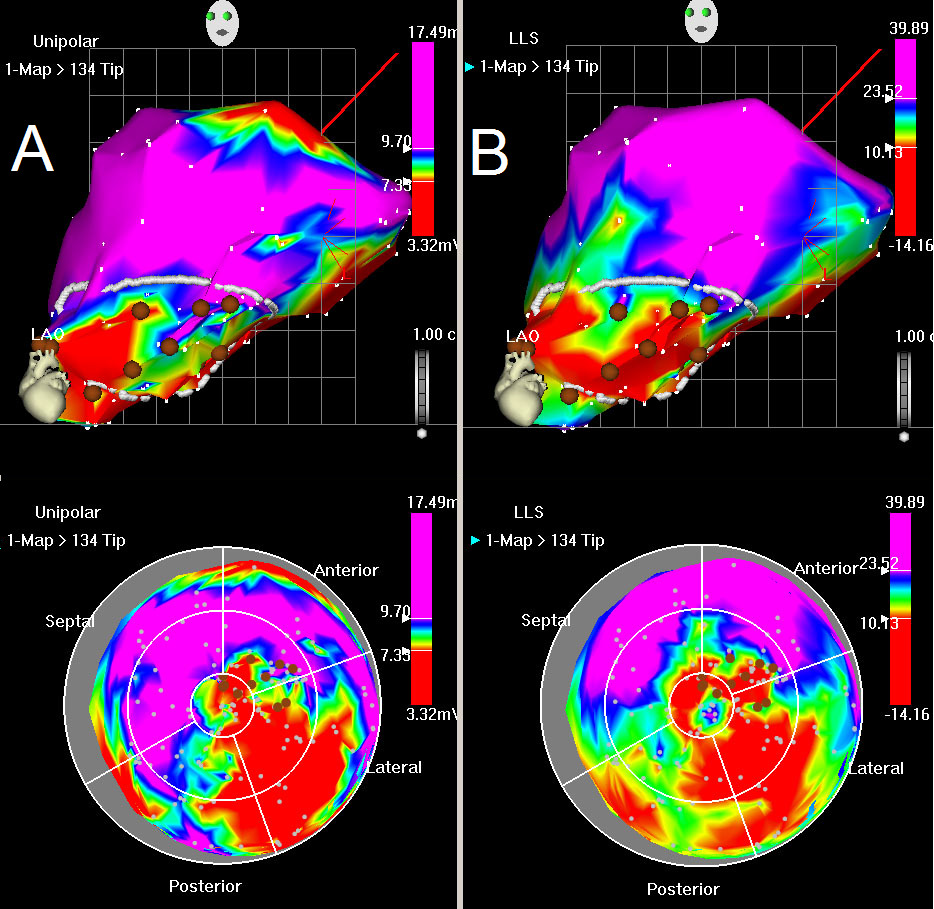
Figure 6: Unipolar voltage and LLS map. (A) Unipolar map, LAO view (top) and bulls eye (below). Red color indicates low unipolar voltage values at myocardial base (normal) with loss of electrical activity posterolateral. Blue indicates normal myocardium, whilst green and yellow colors indicate decreased viability. (B) LLS map, LAO view (top) and bulls eye (below). Red color indicates akinesia in the posterolateral wall, green and yellow indicate decreased wall motion. The mapping points are shown by white dots. The drawn white line shows the area of interest, characterized by decreased unipolar voltages and impaired wall motions. Brown points represent the injection sites.
