The left panels in Figures 9 – 10 are of PN 10 mouse lungs imaged at baseline (pre-instilled). These images show successful instillation of saline challenges into the left lobe of the neonatal lungs. In Figure 9, the mouse lung was tracheally instilled with the saline solution defined above (see section 2.1). The middle and right panels of Figure 9 are X-ray images from the same mouse obtained 5 min and 2 hr post instillation; this animal had successfully cleared the saline challenge. Specifically, the X-ray intensity of this animals ROI increased from 187.67 to 515. Thus, there is a reverse correlation between pixel density and lung fluid volume; that is to say, the larger the relative value, the less fluid there is in the lungs. It may be helpful to understand that more X-ray energy is absorbed (hence a larger reported value) when there is less fluid attenuating the X-ray. In Figure 10, the PN 10 mouse lung was tracheally instilled with a compound containing oxidized glutathione (reconstituted in saline described in 2.1) that inhibited alveolar fluid clearance of the saline challenge by blocking epithelial sodium channel activity; the numerical value of this animal's ROI will decrease from the pre-instill and post-instilled X-ray imaged files, indicative of increasing X-ray opacity. Specifically, the net intensity of the animal approximately 5 min post-instillation was – 64, and decreased to – 182. Again, note the inverse relationship between the ROI pixel intensity and amount of fluid in the lungs; increased fluid in the upper left lobe of the lung attenuates X-ray absorbtion.
Evaluating net intensity of the ROI enables quantitative evaluation of changes in the rate of lung fluid clearance, albeit acquisition software also allows the investigators to express data in terms of g/cm3 if desired. Moreover, the investigators can use each animal as its own control and normalize all X-ray intensities to an initial time point (Io), such as t = 5 min and report net changes in X-ray opacity (i.e., a measure of change in lung fluid volumes).
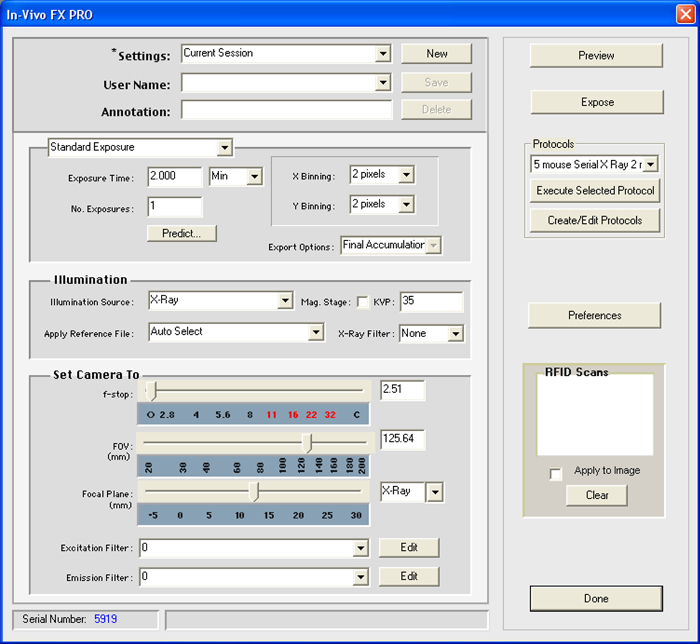
Figure 1. Exposure Settings. This screen shot illustrates the appropriate exposure settings utilized in this protocol. Please click here to view a larger version of this figure.
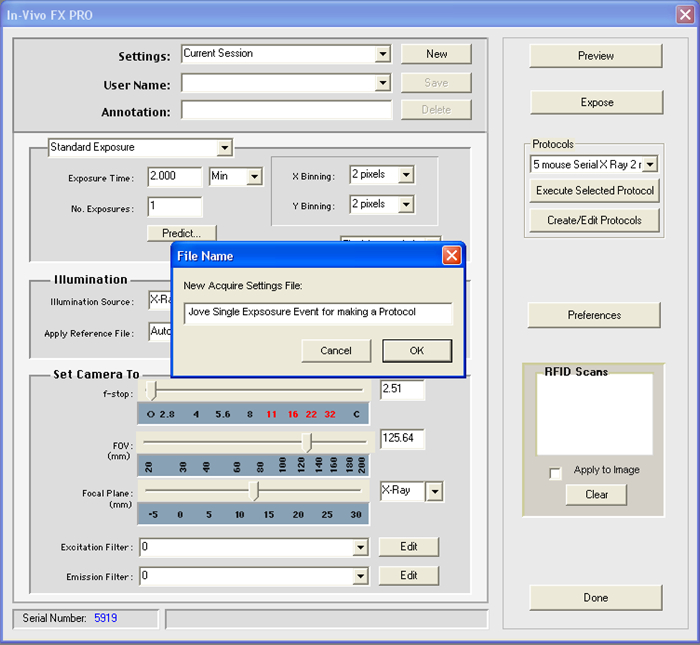
Figure 2. Settings File. This screen shot illustrates a key step in generating a file setting that will be used in a protocol. A pop up window (as shown) will request a new name for the acquisition settings file. Please click here to view a larger version of this figure.
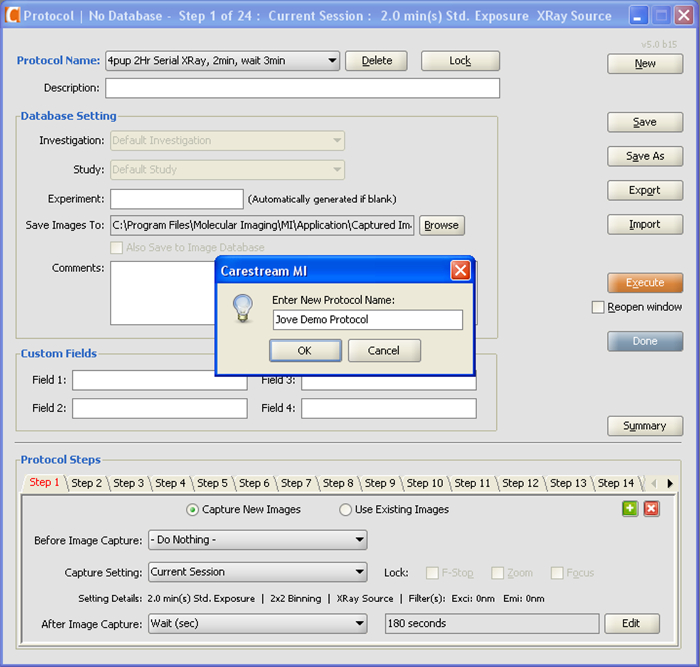
Figure 3. Imaging Protocol. This screen shot illustrates a key step in determining whether a new imaging protocol has been successfully created. A pop up window (as shown) will appear and a new protocol name will be requested for the generated protocol. Please click here to view a larger version of this figure.
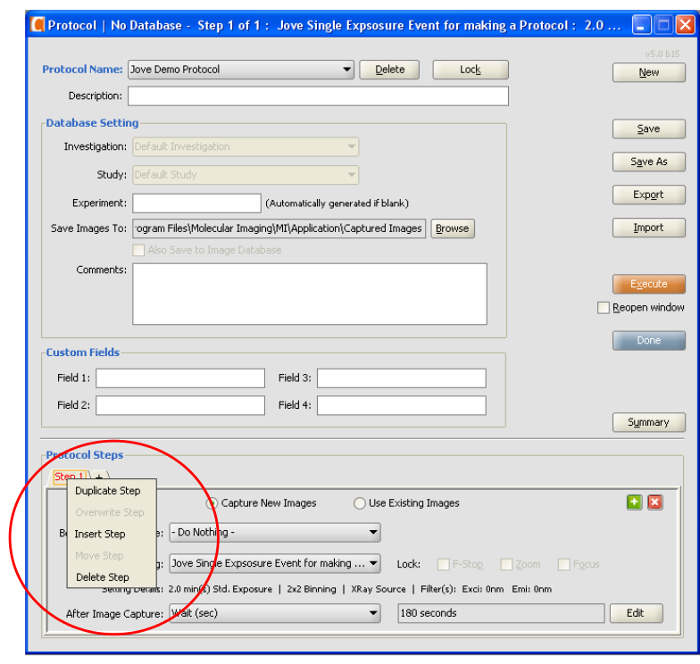
Figure 4. Protocol Steps. This screen shot illustrates a shortcut to duplicate an acquisition settings file, insert a new step, or to delete a step within an imaging protocol. Please click here to view a larger version of this figure.
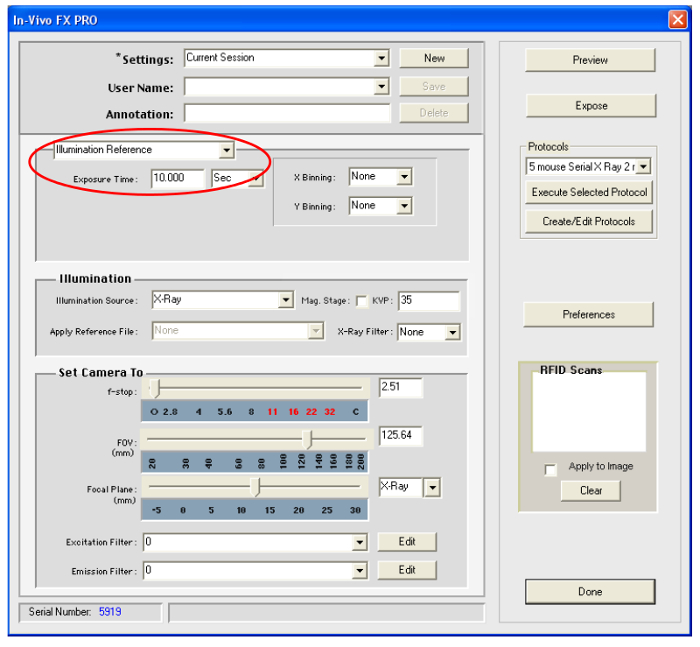
Figure 5. Illumination Reference. This screen shot exhibits the illumination reference command and appropriate settings in the animal imaging software appropriate for creating an illumination reference file. Please click here to view a larger version of this figure.
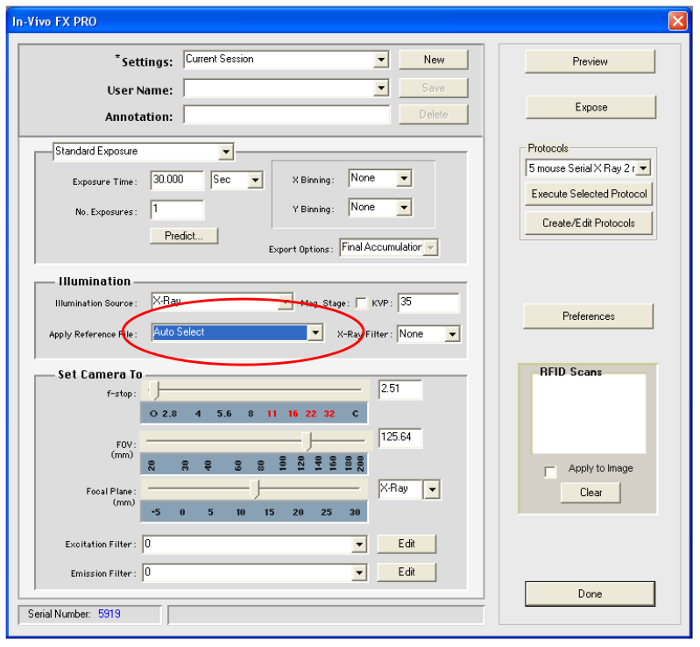
Figure 6. Auto Select. This screen shot exhibits the Auto Select function and appropriate settings in the animal imaging software appropriate for applying an illumination reference file. Please click here to view a larger version of this figure.
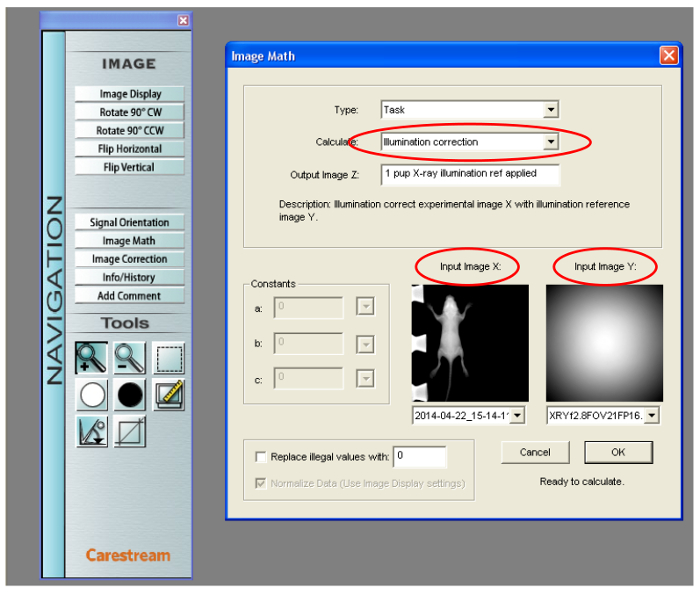
Figure 7. Illumination Correction. This screen shot illustrates the appropriate application of an illumination reference file generated after animal imaging. Please click here to view a larger version of this figure.
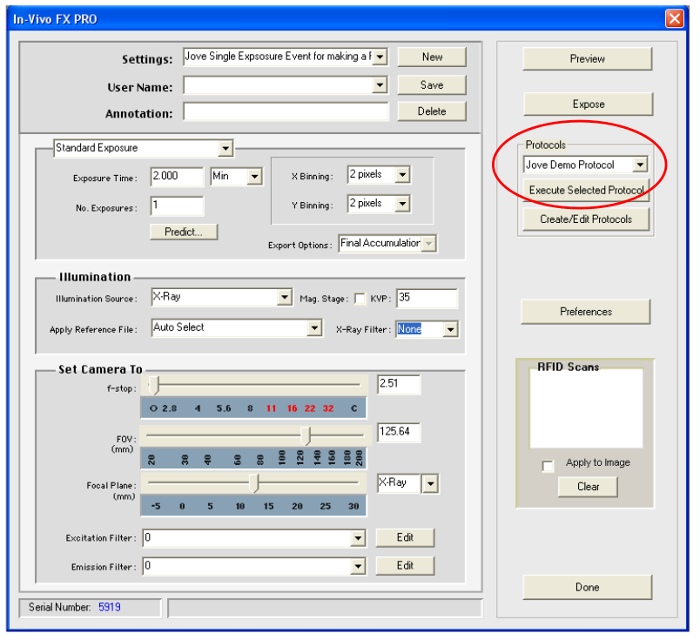
Figure 8. Execute Protocol. This screen shot illustrates how to execute a selected protocol. Please click here to view a larger version of this figure.

Figure 9. X-ray images of cleared lungs. Representative image of PN 10 lungs prior to receiving a saline challenge (pre-instill; left panel); 5 min post-instillation (middle panel), and 2 hr after the saline challenge had cleared from the otherwise healthy lung (right panel). Please click here to view a larger version of this figure.

Figure 10. X-ray Images of Flooded Lungs. Representative image of PN 10 lungs prior to receiving a saline challenge (pre-instill; left panel) containing glutathione disulfide , which inhibits paracellular solute transport; 5 min post-instillation of glutathione disulfide (middle panel), and 2 hr after inhibiting paracellular transport which leads to alveolar flooding (right panel). Please click here to view a larger version of this figure.
| No filter= | 10 sec exposure |
| 0.1mm = | 15 sec exposure |
| 0.2mm = | 20 sec exposure |
| 0.4mm = | 30 sec exposure |
| 0.8mm= | 30 sec exposure |
| The size of the X-ray filter correlates to a specific exposure time for creating an illumination reference file. | |
Table 1. Illumination Reference File. This file reports the appropriate exposure times for generating illumination reference files based on X-ray filters used in imaging studies.
