Two-dimensional laser speckle contrast imaging (LSCI)16 was used to compare the alterations of cerebral blood flow (CBF) by 30 min transient unilateral carotid occlusion (tCCAO), 30 min exposure to hypoxia (7.5% oxygen), and 30 min unilateral carotid ligation under hypoxia (tHI). This experiment revealed that tCCAO under normoxia suppressed the CBF on the carotid ligated hemisphere to ~50% of the baseline value, which quickly recovered to above 85% after release of the carotid occlusion (R in Figure 2A). Exposure to systemic hypoxia alone reduced the CBF to approximately 75% of the baseline value, which transiently rebound to ~130% after returning to the normoxic atmosphere (Figure 2B). In contrast carotid ligation under hypoxia (tHI) quickly reduced CBF in the ipsilateral hemisphere to less than 20% of the baseline value around 10 min, which rarely recovered to above 30% at 20 min after release of the carotid ligation and returning to normoxia. CBF on the contralateral hemisphere (L), however, fluctuated between 20 and 50% during hypoxia, and quickly returned to above 80% after the tHI insult (Figure 2C).
At 24 hr after tCCAo (30 min) or tCCAO plus 30 min hypoxia (tHI), in vivo TTC stain was used to detect infarction17. This analysis showed no obvious injury by the tCCAO insult, but sizable infarction in the middle cerebral artery-supplied territory following tHI insult (Figure 3A). Anti-fibrin(ogen) immunostaining was used to compare the tCCAO- and tHI-injured brains at 1 hour recovery and showed widespread deposition of fibrin(ogen), an indicator of thrombosis, in the tHI-injured, but not tCCAO-challenged mouse brains (Figure 3B, C). Tail-vein injection of Evans blue dye was also used to compare vascular perfusion of tCCAO- and tHI-injured brains at 4 hr recovery. This analysis showed diminished cerebral perfusion and intense extravasation of the Evans blue dye in tHI-injured, but not the tCCAO-challenged mouse brains (Figure 3D, E).
Finally, the outcomes of tHI insult in mice receiving tail-vein injection of vehicle (at 0.5 hr recovery) or recombinant human tPA (Activase, 10 mg/kg, at 0.5, 1, or 4 hours post-tHI) were compared using in vivo TTC stain at 24 hr recovery (Figure 4A). In vehicle-treated mice, the mortality rate at 24 hr post-tHI was 23.8% and only one in 21 tHI-injured mice was beyond the mean and 2 SD (the outlier). The 24 hours mortality rate in mice receiving tPA treatment at 0.5 hr recovery dropped to 8.3%, but this effect was lost when tPA was administrated at 1 or 4 hours after the tHI insult (Figure 4B). Figure 4C plotted the infarct size of all survived mice in the four treatment groups. Of note, both 0.5 and 1 hr tPA-administration significantly reduced infarct size, when compared to vehicle treatment. The 0.5 hr tPA-treatment group also showed a significantly reduced infarct size than the 4 hr tPA-treatment group. Figure 4D showed representative TTC-stain results after each treatment.
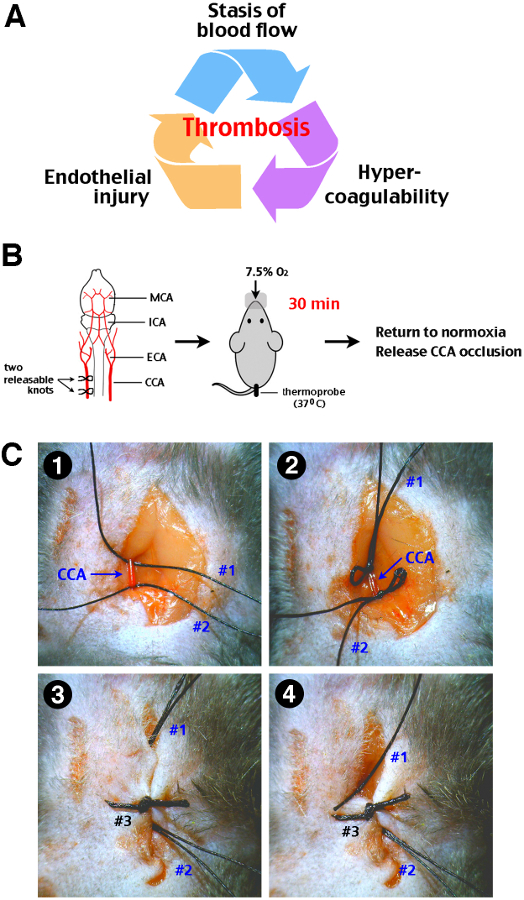
Figure 1: Procedure of transient cerebral hypoxia-ischemia (tHI) insult in adult mice. (A) The Virchow’s triad that propels thrombosis includes stasis of blood flow, endothelial injury, and hypercoagulability of the blood. (B) A schematic diagram of the tHI stroke procedure. Two releasable knots were tied onto the right common carotid artery (CCA), and followed by delivery of 7.5% oxygen via a nose cone for 30 min, while the mouse rectal temperature was maintained at 37-38 °C. After the transient systemic hypoxia, the CCA ligation was released by pulling out one end of the releasable suture knots. MCA, middle cerebral artery; ICA, internal carotid artery; ECA, external carotid artery; CCA, common carotid artery. (C) Surgical procedures for transient right CCA occlusion. 1. Two precut suture (#1 and #2) were placed under an isolated right CAA. 2. Two releasable knots were made. 3. The incision line was closed up by suture #3. Make sure that the ends of suture #1 and #2 were approachable outside the incision line. 4. Carefully pull suture #1 and #2 from outside to release the CCA. When performed gently, this procedure will not cause laceration of the CCA.
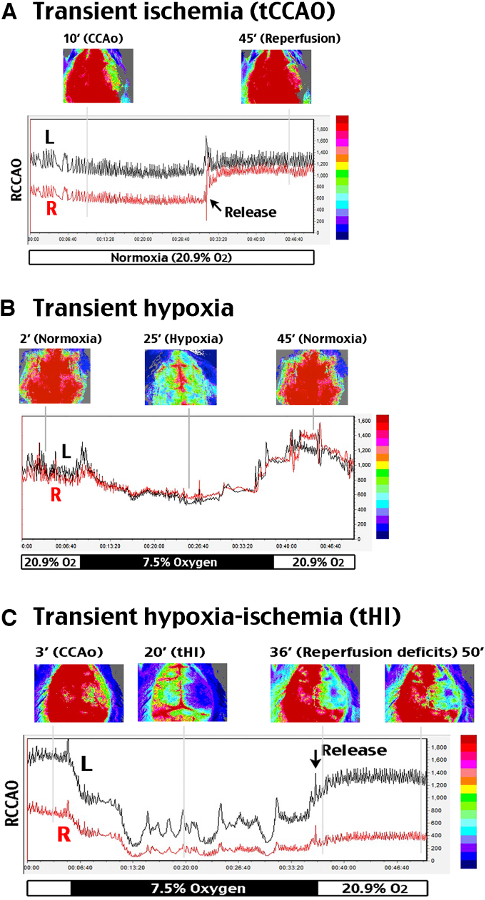
Figure 2: Analysis of cerebral blood flow alterations during and after tHI insult. A two-dimensional laser speckle contrast imaging (LSCI) system was used to evaluate cerebral blood flow (CBF). R (right) indicates the carotid-ligated hemisphere; L (left) is the contralateral hemisphere. (A) tCCAO under normoxia suppressed CBF to ~50% of the baseline value on the carotid-ligated hemisphere (R) for at least 30 min, which recovered to above 85% within 3 min upon release of the carotid ligation. (B) In hypoxia (7.5% oxygen, 30 min) without carotid artery ligation, CBF declined to 76% of the baseline value and transiently rebounded to around 130% after returning to normoxia. (C) In transient carotid ligation under hypoxia (tHI, 30 min), CBF on the carotid-ligated (R) hemisphere quickly dropped to less than 20% of the baseline value, and it rarely recovered to above 30% upon release of the carotid ligation and returning to normoxia. In contrast, CBF on the contralateral (L) hemisphere fluctuated between 20-50% during hypoxia, and quickly returned to >80% of the baseline value after release of carotid ligation and returning to normoxia. Shown are representative CBF tracings for n >4 in each group. The time-points for representative LSCI photographs were marked by grey lines in the representative tracing.
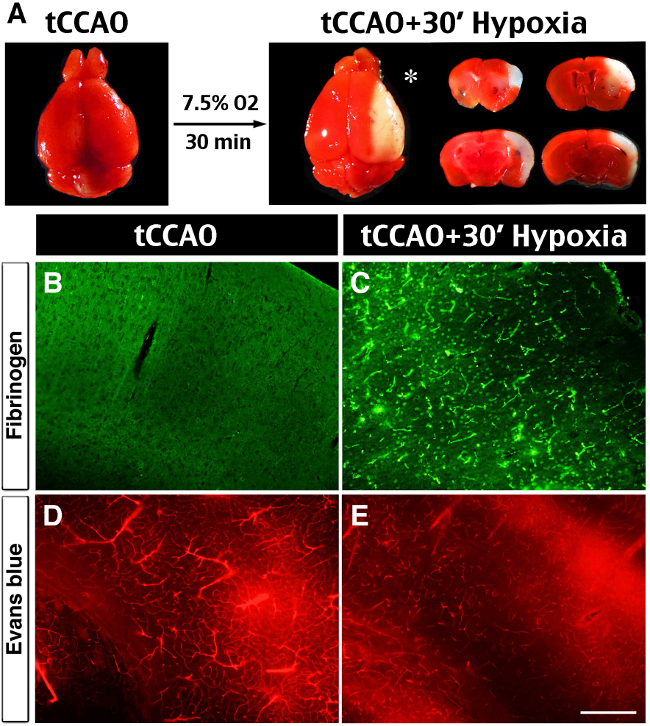
Figure 3: Brain infarct, spontaneous thrombosis and vessel obstruction after the tHI insult. (A) In vivo TTC-stain showed no visible infarction at 24 hr after 30 min transient ligation of the right common carotid artery (tCCAO), but the addition of 30 min hypoxia (7.5% oxygen) to tCCAO produced sizeable infarction in the ipsilateral hemisphere (asterisk), mostly in the middle cerebral artery-supplying area. (B, C) Anti-fibrin(ogen) immunostaining at 1 hr after the tHI insult showed widespread deposits in the ipsilateral hemisphere. In contrast, there was no fibrin(ogen) deposits at 1 hr after the tCCAo (30 min) insult (n >4 for each). (D, E) Cerebral perfusion was evaluated by tail-vein injection of Evans Blue dye at 4 hr after tCCAO (30 min) or tHI (30 min) insult. In post-tCCAO brain, Evans Blue dye filled most of the blood vessels in the ipsilateral hemisphere. In contrast, in post-tHI brain, Evan Blue dye filled fewer blood vessels and was leaked into the parenchyma (n >3). Scale bar: 250 μm.
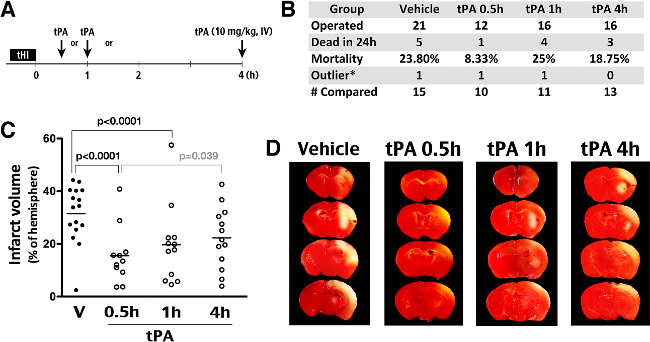
Figure 4: Effects of tPA thrombolysis in the tHI stroke model. (A) Outline of experiments to compare the effects of intravenous tPA administration (10 mg/kg) at 0.5, 1, or 4 hr after the tHI insult. (B) Summary of the number of operated animals, mortality in 24 hr after insults, outliers (the infarct size outside the mean +/- 2 SD), and the number of animals included for comparison of the infarct size. (C) Quantification showed an averaged 32% infarct volume in the vehicle group and significant reduction of infarction in the 0.5 hr (to 16%) and 1 hr (to 20%) groups (Shown are the mean and SEM for each group). The p-values are determined by t-test. (D) Representative TTC-stained brain from animals that were challenged by the tHI insult and received tPA treatment at the indicated time-point after injury. In TTC staining, live tissue showed red color; infarct tissue was pale.
