Standardized MIC methods are necessary in order to monitor resistance development, an important goal of various antimicrobial surveillance programs. Dalbavancin MIC results for isolates collected in Europe and USA in 2011-2013 were <0.25 µg/ml for 99.9% of S.aureus and 100% of streptococci (Table 4).
To assess the importance of using fresh (sealed) DMSO, triplicate testing of dalbavancin BMD MICs for QC strains S. aureus ATCC 29213, and E. faecalis ATCC 29212 and duplicate testing for S. pneumoniae ATCC 49619 was performed using (1) DMSO from sealed ampules, (2) DMSO from a 1 L bottle that was within the expiration date and had been used previously for 2 years and (3) an aliquot of DMSO from the same 1 L bottle (sample 2) that was allowed to sit in an open beaker for 72 hr prior to use. Dalbavancin MIC results using panels made with all three DMSO samples were similar and within the acceptable QC ranges (Table 5).
The loss of dalbavancin activity following exposure of the stock solution to plastic and without the addition of P-80 has been well documented7. In 2 additional studies, the addition of P-80 to the initial and intermediate stock solutions (Table 6) and the use of glass or plastic tubes for the preparation of the initial and intermediate stock solutions (Table 7) did not have an effect on the dalbavancin MIC results. There was also no effect on dalbavancin MIC results when polypropylene and polystyrene plates from three manufacturers were used (Table 7).
The presence of lysed horse blood in the broth media for testing of streptococci has been shown to have a surfactant-like activity, comparable to P-807, 8. The dalbavancin reference method for streptococcus does include both P-80 and lysed horse blood, however, unlike staphylococci and enterococci, dalbavancin MIC results for streptococci are similar (within +/- 1 dilution) with and without the addition of P-80.
As has been previously presented and shown in Figure 1, dalbavancin agar dilution (AD) MICs are typically 2-8 fold higher compared to the current BMD reference12, 13, 14. Unlike BMD, the addition of 0.002% P-80 does not affect dalbavancin AD MIC results12.

Equation 1: Example of Dalbavancin Stock Solution Preparation. Preparation steps for 25 ml of 800 µg/ml dalbavancin solution.
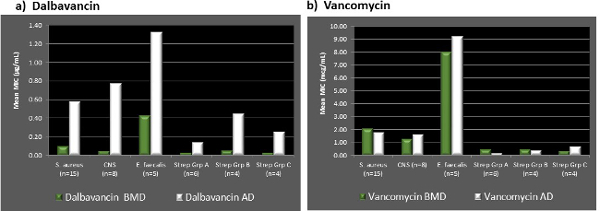
Figure 1. Comparison of Dalbavancin and Vancomycin BMD to AD. Results of study that compared dalbavancin and vancomycin BMD and AD MIC results for select Gram-positive bacterial isolates. Average (A) Dalbavancin and (B) Vancomycin Broth Microdilution and Agar Dilution MIC Results in µg/ml for 15 Staphylococcus aureus, 8 Coagulase Negative Staphylococci (CNS), 5 Enterococcus faecalis and 14 Streptococci (Groups A, B, and C). Please click here to view a larger version of this figure.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
| A | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| B | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| C | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| D | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| E | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| F | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| G | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| H | DAL 0.002 | DAL 0.004 | DAL 0.008 | DAL 0.015 | Dal 0.03 | DAL 0.06 | DAL 0.12 | DAL 0.25 | DAL 0.5 | DAL 1 | DAL 2 | Pos Ctrl. |
| DAL | Dalbavancin | |||||||||||
| Concentrations are stated in µg/ml after 50 µl/well inoculation | ||||||||||||
Table 1. MIC Plate Format. The 96 well plate format showing location of dalbavancin dilutions and positive control wells used as an example in this video publication
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
| Source Conc. (µg/ml) | Volume Source (ml) | Volume DMSO (ml) | Intermediate Conc. in DMSO (µg/ml) | Volume Intermediate Conc. (ml) | Volume CAMHB + 0.004% P80* (ml) | 2X Conc. After 1:100 Dilution in CAMHB (µg/ml) | Final Panel Conc. Post Inoculation (µg/ml) |
| 800 | 1.0 | 1.0 | 400 | 0.02 | 1.98 | 4 | 2 |
| 400 | 0.5 | 0.5 | 200 | 0.02 | 1.98 | 2 | 1 |
| 400 | 0.5 | 1.5 | 100 | 0.02 | 1.98 | 1 | 0.5 |
| 400 | 0.5 | 3.5 | 50 | 0.02 | 1.98 | 0.5 | 0.25 |
| 50 | 0.5 | 0.5 | 25 | 0.02 | 1.98 | 0.25 | 0.125 |
| 50 | 0.5 | 1.5 | 12.5 | 0.02 | 1.98 | 0.125 | 0.06 |
| 50 | 0.5 | 3.5 | 6.25 | 0.02 | 1.98 | 0.06 | 0.03 |
| 6.25 | 0.5 | 0.5 | 3.13 | 0.02 | 1.98 | 0.03 | 0.015 |
| 6.25 | 0.5 | 1.5 | 1.5 | 0.02 | 1.98 | 0.015 | 0.008 |
| 6.25 | 0.5 | 3.5 | 0.8 | 0.02 | 1.98 | 0.008 | 0.004 |
| 0.8 | 0.5 | 0.5 | 0.4 | 0.02 | 1.98 | 0.004 | 0.002 |
| This table has been modified from CLSI M100-S25, Table 8B3 | |||||||
Table 2. Scheme for Preparing Dilutions of Water-Insoluble Antimicrobial Agents to be Used in Broth Dilutions Susceptibility Testing. Volumes of dalbavancin working solutions and diluents for preparation of final MIC dalbavancin solutions of 0.002-2 µg/ml.
| Quality Control Strain | Expected Dalbavancin MIC (µg/ml) |
| S. aureus ATCC 29213 | 0.03-0.12 |
| E. faecalis ATCC 29212 | 0.03-0.12 |
| S. pneumoniae ATCC 49619 | 0.008-0.03 |
Table 3. Expected Dalbavancin MIC Results for Quality Control Strains3, 11. CLSI quality control results for suggested strains to be tested along with clinical isolates in order to verify proper methodology
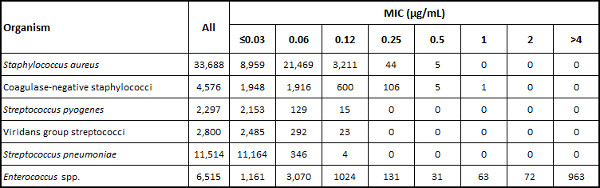
Table 4. Distribution of Dalbavancin MIC Results (Number at each MIC) from USA and European 2011-2013 Surveillance Study15. Dalbavancin MIC results from a published study of recent clinical isolates as an indicator of current dalbavancin in vitro activity.
| Isolate # | Dalbavancin MIC (µg/ml) | ||
| DMSO 1 | DMSO 2 | DMSO 3 | |
| S. aureus ATCC 29213 | 0.12 | 0.06 | 0.06 |
| 0.12 | 0.06 | 0.06 | |
| 0.06 | 0.06 | 0.06 | |
| E. faecalis ATCC 29212 | 0.06 | 0.06 | 0.06 |
| 0.06 | 0.06 | 0.06 | |
| 0.06 | 0.06 | 0.06 | |
| S. pneumoniae ATCC 49619 | 0.015 | 0.015 | 0.015 |
| 0.03 | 0.015 | 0.015 | |
| DMSO 1 = Unopened flame sealed 10 ml ampules | |||
| DMSO 2 = Frequently opened 1L bottle | |||
| DMSO 3 = Frequently opened 1L bottle – sat on bench in uncovered beaker for 72 hr | |||
Table 5. Dalbavancin MIC Results (µg/ml) using DMSO Stock and Intermediate Dilutions Preparation with DMSO from 3 Sources. Results of a dalbavancin MIC study that compared effect of using different DMSO solvents in preparation of the dalbavancin stock and intermediate dilutions.
| Isolate Number | Replicate Number | Dalbavancin MIC (µg/ml) | |
| DALB w/P80 in DMSO | DALB w/o P80 in DMSO | ||
| S. aureus ATCC 29213 | 1 | 0.06 | 0.06 |
| 2 | 0.06 | 0.06 | |
| 3 | 0.06 | 0.06 | |
| 4 | 0.06 | 0.06 | |
| S. aureus clinical DP80-002SA | 1 | 0.03 | 0.03 |
| S. aureus ATCC 700699 | 1 | 0.5 | 0.5 |
| S. pneumoniae ATCC 49619 | 1 | 0.03 | 0.015 |
| 2 | 0.03 | 0.015 | |
| 3 | 0.03 | 0.015 | |
| 4 | 0.03 | 0.015 | |
| S. pyogenes clinical: | |||
| DP80-004PY | 1 | 0.015 | 0.015 |
| DP80-005PY | 1 | 0.03 | 0.03 |
| DP80-006PY | 1 | 0.03 | 0.015 |
| DP80-007PY | 1 | 0.06 | 0.03 |
| DP80-008PY | 1 | 0.03 | 0.015 |
| S. agalactiae clinical: | |||
| DP80-009AG | 1 | 0.06 | 0.12 |
| DP80-010AG | 1 | 0.06 | 0.03 |
| DP80-011AG | 1 | 0.06 | 0.06 |
| DP80-012AG | 1 | 0.06 | 0.06 |
| S. dysgalactiae clinical DP80-013DY | 1 | 0.03 | 0.03 |
| S. pneumoniae clinical: | |||
| DP80-014SP | 1 | 0.06 | 0.06 |
| DP80-015SP | 1 | 0.03 | 0.03 |
| DP80-016SP | 1 | 0.03 | 0.03 |
| DP80-017SP | 1 | 0.06 | 0.06 |
Table 6. Dalbavancin MIC Results using DMSO Stock and Intermediate Dilutions Preparation with and without 0.002% P-80. Results of a dalbavancin MIC study that compared effect of adding 0.002% P-80 to dalbavancin stock and intermediate dilutions.
| Isolate | Replicate Number | Stock Dilution Tubes | Microtiter Plate (Plastic Type) | ||||||
| Poly-propylene, Greiner | Polystyrene | ||||||||
| Glass | Plastic | Plastic 1hr | Plastic 1hr / Intermediate 1hr | Greiner | Corning | Nunc | |||
| S. aureus ATCC 29213 | 1 | 0.06 | 0.03 | 0.03 | 0.03 | 0.06 | 0.03 | 0.06 | 0.03 |
| 2 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.06 | |
| 3 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | 0.03 | |
| E. faecalis ATCC 29212 | 1 | 0.06 | 0.06 | 0.06 | 0.06 | 0.03 | 0.03 | 0.06 | 0.03 |
| 2 | 0.06 | 0.06 | 0.06 | 0.06 | 0.03 | 0.03 | 0.06 | 0.03 | |
| 3 | 0.06 | 0.06 | 0.06 | 0.06 | 0.03 | 0.03 | 0.06 | 0.03 | |
| S. pneumoniae ATCC 49619 | 1 | 0.015 | 0.015 | 0.015 | 0.015 | 0.008 | 0.008 | 0.008 | 0.008 |
| 2 | 0.015 | 0.015 | 0.015 | 0.015 | 0.008 | 0.015 | 0.008 | 0.008 | |
| Glass = Initial stock made in glass bottle, used immediately to make intermediate concentrations in plastic tubes, used immediately to make broth dilutions. | |||||||||
| Plastic = Initial stock made in plastic centrifuge tube, used immediately to make intermediate concentrations in plastic tubes, used immediately to make broth dilutions. | |||||||||
| Plastic 1 hr = Initial stock made in plastic centrifuge tube, let sit on bench for 1 hr then used to make intermediate concentrations in plastic tubes, used immediately to make concentrations in broth. | |||||||||
| Plastic 1 hr / Intermediate 1 hr = Initial stock made in plastic centrifuge tube, let sit on bench for 1 hr then used to make intermediate concentrations in plastic tubes, let sit on bench for 1 hr then used to make concentrations in broth. | |||||||||
Table 7. Dalbavancin MIC Results using Stock Dilutions Preparation in Plastic and Glass Tubes and MIC Plate Plastic Types. Results of a dalbavancin MIC study that compared effect of using plastic or glass tubes when preparing the stock solutions and also effect of using different sources and types of plastic for microtiter plates.
