An Improved Method for Rapid Intubation of the Trachea in Mice
Summary
This article presents a rapid and simple method for administering bleomycin directly into the mouse trachea via intubation. Key advantages of this method are that it is highly reproducible, easy to master, and does not require specialized equipment or lengthy recovery times.
Abstract
Despite some anatomical and physiological differences, mouse models continue to be an essential tool for studying human lung disease. Bleomycin toxicity is a commonly used model to study both acute lung injury and fibrosis, and multiple methods have been developed for administering bleomycin (and other toxic agents) into the lungs. However, many of these approaches, such as transtracheal instillation, have inherent drawbacks, including the need for strong anesthetics and survival surgery. This paper reports a quick, reproducible method of intratracheal intubation that involves mild inhaled anesthesia, visualization of the trachea, and the use of a surrogate spirometer to confirm exposure. As a proof of concept, 8-12 week old C57BL/6 mice were administered either 2.0 U/kg of bleomycin or an equivalent volume of PBS, and both damage and fibrotic endpoints were measured post-exposure. This procedure allows researchers to treat a large cohort of mice in a relatively short period with little expense and minimal post-procedure care.
Introduction
In spite of some anatomical and physiological differences,1 murine models continue to be invaluable for modeling human biology and disease pathogenesis.2 From a husbandry standpoint, mice are easy to handle, have a low breeding time, an accelerated lifespan, and are relatively inexpensive to house. With the development of diverse genetic strains and strategies (e.g., conditional knock-outs, reporter mice, lineage-tracing approaches, etc.), as well as the wide range of available reagents (e.g., antibodies, recombinant proteins, inhibitors, etc.), mice have become an essential model vertebrate organism to uncover human homeostasis and disease processes.3
Mice have been especially valuable for studying pulmonary conditions, including acute lung injury (ALI) and pulmonary fibrosis.4 ALI in humans can be caused by trauma, injury, or sepsis and is characterized by epithelial and endothelial leak (i.e., edema), inflammation, and nascent fibrosis. In many patients, ALI progresses to its severe form, acute respiratory distress syndrome (ARDS), which often results in fibrosis and death due to respiratory failure.5,6 Pulmonary fibrosis is a progressive, fatal pathology characterized by the excess deposition of extracellular matrix, most notably type I collagen, leading to impaired lung function.7,8 Administration of bleomycin (BLM) is the most widely used and best characterized model for inducing ALI and fibrosis in experimental animals.9 Although BLM-induced pulmonary fibrosis in rodents does not recapitulate fully the human fibrotic phenotypes,10 mouse studies with this model have led to the discovery of many important factors influencing the onset and progression of disease.11
While the exact mechanism(s) behind BLM-induced fibrogenesis are unknown, the initiating injury is thought to arise from contact-dependent DNA strand breaks in the epithelial cells lining the conducting airways and alveoli, and in particular, type 1 pneumocytes.12 The need for direct contact between BLM and the pulmonary epithelium highlights the importance of a robust delivery route, and these concerns are also germane to a broad range of treatments targeted to the distal airways, including recombinant proteins, antibodies, siRNA, virus, bacteria, particulates, and more. Oropharyngeal aspiration (OPA) has been widely used for this purpose13, but a major a shortcoming of OPA is that some portion of the delivered agent may be swallowed into the gastrointestinal tract, thereby leading to imprecision in the administered dose. Another widely used approach is transtracheal instillation, which involves tracheostomy under strong anesthesia to expose the trachea and instillation of an agent directly into the respiratory tract.14 However, not only may such a procedure be undesirable due to its invasivity, but it is also time consuming, requires a fair bit of training, and causes a potent injury to the respiratory tract.15,16 Several protocols have been developed that involve the direct administration of agents into the trachea without the need for surgical intervention,16,17,18,19,20 but these methods involve extended recovery times caused by powerful anesthetics, the use of expensive equipment (i.e., otoscope/laryngoscope, commercially available procedure boards, fiber-optic wires, etc.), an excess of manipulation in the oral cavity, and uncertainty regarding the dosage.
This paper describes a relatively easy method of administration via intubation that allows a researcher to quickly, inexpensively, and reliably instill a reagent into the murine lung with limited risk of residual damage to the surrounding tissues.
Protocol
The Institutional Animal Care and Use Committees (IACUC) at the University of Washington and Cedars-Sinai Medical Center have approved the animal work necessary for these studies.
1. Preparation
- Sterilize both the blunt end forceps and the depressor via autoclave.
- Using a biological safety cabinet, prepare a working stock of BLM in PBS from the lyophilized powder. Sonicate the solution for 10 min at 35 Khz to assure even mixing.
Note: A total volume of between 30 and 45 µl is recommended to prevent pipetting variation on the low end, and suffocation with larger volumes. - Prepare a clean workspace that includes approximately 1 m2 for the procedure itself, as well as designated locations for cages both before and after the procedure.
- Fix the base of the procedure board to the bench immediately in front of the researcher by laying 2 or 3 strips of laboratory tape across the base and underlying bench. See Figure 1 for further specifications on creating a board.
- Tie a single length of size 4.0 suture thread between the two positioning screws of the procedure board.
- Generate a makeshift spirometer by removing and discarding the plunger from three 1 ml syringes, and depositing 60 µl of PBS into the top of each barrel to form an airtight seal. Secure the hub of the catheter loosely to one of the syringes and place it to one side of the board.
- Aspirate 300 µl of air into a 1 ml syringe and place it to one side of the board.
- Cut an additional piece of tape approximately 6 inches in length and place to one side. This will be used to secure the animal to the board in step 2.4.
- Set up an isoflurane chamber. Attach O2, isoflurane, and vacuum to the appropriate ports on both the exposure chamber and the clearance vacuum. Alternatively, administer anesthetic in an isoflurane-compatible biological safety cabinet.
2. Intubation
- Anesthetize the mouse with isoflurane in the chamber until it loses consciousness and respiration slows to an appropriate rate. A typical exposure includes 4% isoflurane and 2% O2 for 3 to 4 min, and the ideal outcome is 2 to 2.5 min of sedation. This corresponds to a respiration rate of 1 breath every 2 sec.
- While waiting for sedation to set in, aspirate between 30 and 45 µl of BLM into a pipettor and place to one side.
- When ready, suspend the sedated mouse by its upper incisors from the thread attached to the positioning screws of the procedure platform. Make sure that the animal's dorsum lies flat against the platform surface.
- Being careful not to restrict ventilation, place a piece of tape loosely across the lower (caudal) portion of the thoracic cavity, just above the diaphragm. Placement should be tight enough to maintain proper alignment during the procedure, but not so tight that it restricts respiration.
- Turn on the illuminator to between 80% and 100% intensity and orient the gooseneck so that it is 1 to 2 cm from the surface of the skin, near the solar plexus. Periodically check the tip of the gooseneck for heat to ensure that it does not injure the mouse.
- Standing behind the platform, use the sterile, blunt end forceps to locate the tongue. Being careful to avoid the lower incisors, gently grip and draw the tongue out of the oral cavity.
- Using the remaining hand, insert the depressor and use it to flatten the tongue against the floor of the oral cavity. Release the forceps, but leave the depressor in place for the next two steps.
- Orient the light so that the trachea is visible by guiding the gooseneck proximally from the level of the solar plexus until it reaches the level of the mainstem bronchi.
Note: The trachea can be easily distinguished by the action of respiration, which causes the emitted light to fluctuate in intensity. When correctly positioned, this structure will be discernable in the axial plane as a centrally located pin of light with minimal ambient light in the oral cavity itself. - Angle the syringe so that it follows the natural path of the trachea, and lower the 22-G catheter tip, with the attached syringe containing the droplet, straight into the lumen. The PBS bubble will begin to rise and fall with each breath upon successful placement.
Note: This action may be delayed by several seconds as a result of deep sedation. - Feed the catheter in an additional 5 mm. Remove the tongue depressor.
- Shift the syringe to the opposite hand, and gripping the hub, gently remove the syringe.
- Deposit between 30 and 45 µl of BLM into the center of the interior of the catheter hub, attach the second syringe and dispense 300 µl of air into the hub.
- Replace the second syringe with the first containing the bubble of PBS. The bubble will continue to rise and fall if the procedure has been performed successfully.
3. Post-procedural Care
- Remove the catheter and tape, and place the animal in a dry warm place until it regains consciousness – typically within a couple of minutes.
Representative Results
Intubated mice were monitored daily for weight loss and distress, and sacrificed 4, 10 or 17 days later via intraperitoneal injection of 2.5% 2,2,2-tribromoethanol. Bronchoalveolar lavage (BAL) was collected in three washes of PBS as described elsewhere 21, and the right lung was fixed in 10% formalin, paraffin embedded, and stained with Masson's Trichrome by the University of Washington Histology and Imaging Core 22.
In keeping with established data, BLM-treated mice experienced peak weight loss between days 7 and 10 post exposure 23 (Figure 2A). In addition, elevated levels of IgM in BAL from sacrificed BLM-treated mice demonstrated a significant, time-dependent increase in lung permeability, indicative of epithelial and/or endothelial barrier dysfunction (Figure 2B).
The fibrogenic response was measured using Masson's trichrome stain – a well-established marker of total collagen content 24. Right lungs were stained, and the average total area of trichrome staining per right lung section was quantified (Figure 3A). Representative sections show the resulting treatment-dependent thickening of the pulmonary interstitium and increases in fibrotic lesions (Figure 3B).
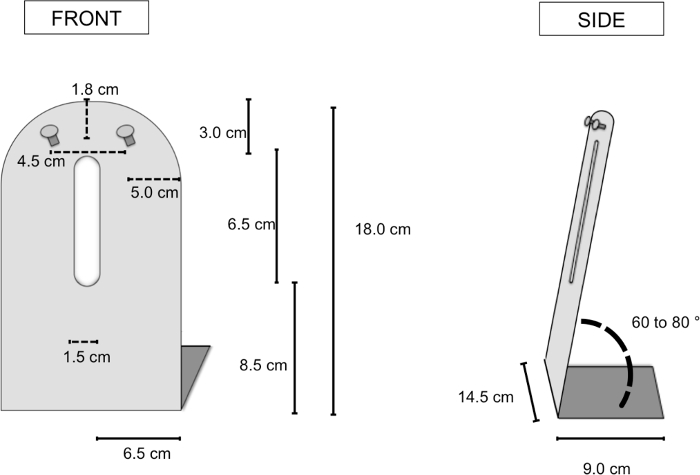
Figure 1. General parameters for producing a working procedure board. The lengths presented indicate the approximate dimensions necessary for creating a working procedure apparatus. In these experiments, standard aluminum sheet metal was cut to the proper dimensions, then reinforced with a "T" bracket. Please click here to view a larger version of this figure.
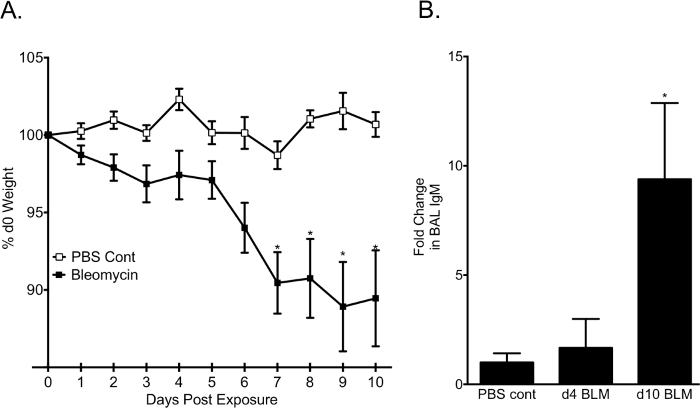
Figure 2. Weight loss and barrier dysfunction following administration of bleomycin. Mice were administered 2.0 U/kg of BLM or an equal volume of PBS. (A) Weight loss expressed as percentage of day 0 weight (BLM: n=21; PBS: 5). (B) Mice were sacrificed at 4 or 10 days post-exposure, and IgM protein in BAL from harvested lungs was measured via ELISA. (PBS: n=5; day 4: n=3; day 10: n=5). Data are presented as mean ± SEM. * P<0.05 compared to PBS control. Please click here to view a larger version of this figure.
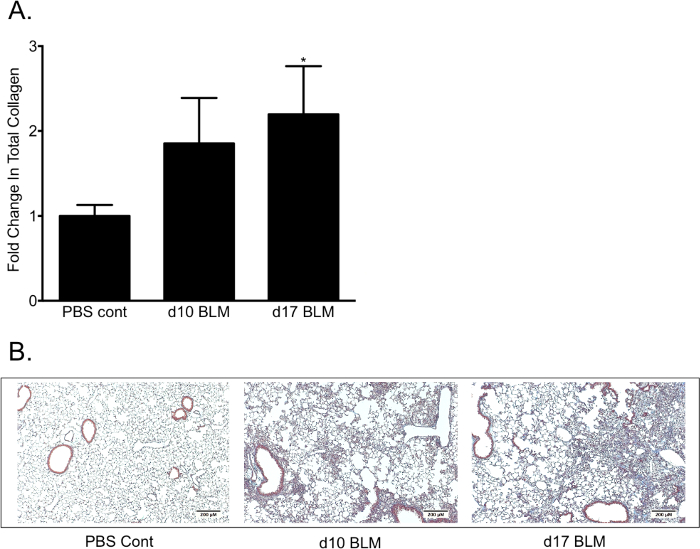
Figure 3. Pulmonary fibrosis following administration of bleomycin. (A) Total collagen, quantified as total fold change Masson's trichrome staining from WT controls. (B) Representative images of trichrome stained lung sections taken at 5x magnification. PBS control consists of animals taken between 5 and 14 days post-PBS treatment (PBS: n=5; day 10: n=5; day 17: n=3). Data are presented as mean ± SEM. * P<0.05 compared to PBS control. Please click here to view a larger version of this figure.
Discussion
In instances where aerosolization is impractical due to limited reagent availability, safety, or cost, direct tracheal administration is a superior method for delivery of exogenous agents into the lungs.16 Transtracheal instillation has been widely used to accomplish this; however, as with all surgical intervention, it also carries with it the potential for complications caused by the procedure itself, and not necessarily the agent being instilled.13 For these reasons, it has become increasingly common to administer a substance directly into the trachea via intubation16,17,18,19,20. However, these methods also suffer from limitations, including extended recovery times due to the use of powerful sedatives like ketamine/xylazine, uncertainty regarding the placement of the catheter (i.e., into the esophagus and not the trachea), unnecessary manipulation of tissues in the oral cavity, and the cost associated with purchasing specialized instruments such as otoscopes/laryngoscopes.
Once established, the approach outlined here provides several meaningful benefits over other intubation protocols. For one thing, the use of isoflurane allows for a reduction in the total time expended per mouse. This is primarily due to the reduced time needed for animals to regain consciousness following isoflurane sedation compared to controlled substances like ketamine (about 5 min versus sometimes greater than 3 hr).14 In addition, the makeshift spirometer ensures confidence of success by allowing the researcher to visualize the oscillating PBS bubble, which indicates correct placement of the administered substance both before and after instillation. Finally, by utilizing an external light source instead of a bulky otoscope or laryngoscope and guide wire, the researcher is able to reduce the amount of equipment in their hands, while simultaneously improving their view of the oral cavity and reducing their chances of damaging the soft tissues surrounding the trachea.
Specific concerns associated with this protocol are few, but serious. For example, while the use of isoflurane reduces the time associated with induction and recovery from sedation, it also requires rigorous observation of the animal's sedation state. Failure to remove the animal from the isoflurane chamber in a timely manner can result in death, especially in animals already recovering from a previous intervention. Conversely, insufficient isoflurane dosage and extended procedural times can result in the animal regaining consciousness during the procedure itself, which can also result in injury. Therefore, it is imperative for both the safety of the animal and the integrity of the experiment that the animal be returned to the isoflurane chamber at the first sign of consciousness. Since this can be common when learning this method, it is recommended that inexperienced researchers confirm successful administration of each animal before anesthetizing the next. In addition, researchers having difficulty can also choose to extend the isoflurane exposure to increase the available procedural time, provided that they closely monitor the animals for moribundity.
An additional concern of this method is that of damage associated with handling. This is especially likely during three steps: when removing the tongue from the mouth, when inserting the catheter, and when dislodging the syringes from the hub following treatment. The catheter placement is by far the most hazardous of these steps. Importantly, the catheter should not enter the oral cavity until the view of the trachea is ideal. If the trachea cannot be brought into view through manipulation of either the light source or the depressor, the researcher should release the tongue and reattempt the procedure. Manipulation of the soft tissues surrounding the trachea is not necessary or recommended. However, once the catheter has been correctly placed, care should also be taken to keep the hub from advancing too far into the trachea and perforating the main-stem bronchi. This can generally be avoided by ensuring that the catheter is only loosely attached to the syringe barrel, and by bracing the hand containing the catheter against the procedural board so that it remains static. These nuances, together with the need for timeliness and precision, highlight the importance of preparation and practice in perfecting this procedure. Nevertheless, with training it should be possible for a novice researcher to treat 20 or more animals over the course of an hour, and for experienced researchers to complete twice as many or more.
The consistency imparted by direct tracheal deposition has made it a preferred route of administration in recent years. In fact, similar methods have already been reported for a multitude of disparate materials in this way 19,25. Consistent with such protocols, delivery of bleomycin in the manner outlined here resulted in a potent fibrotic response in both lungs, and in all lobes, suggesting a similar level of depth and uniformity in distribution. Based on this, it is probable that this protocol provides comparable experimental advantages for a range of other materials that rely on contact to mediate their effects (e.g., pharmaceuticals, antibodies, bacterial agents, and in vivo protein modification systems such as lentiviral vectors), and that, like bleomycin, it would allow such experiments to also be conducted with confidence, little expense, and minimal post-operative care.
Declarações
The authors have nothing to disclose.
Acknowledgements
The authors thank Brian Johnson of the Histology and Imaging Core at the University of Washington for help with the trichrome staining and analysis. This work was supported by NIH grants HL098067 and HL089455.
Materials
| Bleomycin For Injection, 30 units/vial | APP Pharmaceuticals, LLC | 103720 | For best results, BLM should be suspended in PBS, aliquoted, and stored as single use lyophilzed aliquots |
| Blunt End Forceps | N/A | N/A | |
| Tongue Depressor (i.e. bent Valleylab Blade Electrode, 2.4") | Covidien | E1551G | Before use, create a 45 degree bend 1.5 cm from the blade tip. A suitable depressor can also be created from any metal implement of similar dimensions. |
| Exel Safelet Catheter 22G X 1" | Exel International | 26746 | |
| 1 mL Slip-tip Disposable Tuberculin Syringe (200/sp, 1600/ca) | BD | 309659 | |
| 0.2ml Pipettor and Filter Tips | N/A | N/A | |
| Fiber-Lite Illuminator. Model 181-1: Model 180 mated with Standard Dual Gooseneck illuminator | Dolan Jenner Industries, Inc. | 181-1 | Lower output LED illuminators are not recommended as they fail to suficiently illuminate the trachea. |
| Intubation Board | N/A | N/A | See Diagram 1. |
| Colored Label Tape: 0.5 in. Wide | Fisherbrand | 15-901-15A | |
| Oxygen | N/A | N/A | |
| Phosphate-Buffered Saline, 1X | Corning | 21-040-CV | Product should be sterile |
| Non-Sterile Silk Black Braided Suture Spool, 91.4 m, Size 4-0 | Harvard Apparatus | 517698 | |
| Table Top Anesthesia Machine Isoflurane | Highland Medical Equipment | N/A | http://www.highlandmedical.net/ |
| Slide Top Induction Mouse Isoflurane Chamber | MIP / Anesthesia Technologies | AS-01-0530-SM | |
| FORANE (isoflurane, USP) Liquid For Inhalation 100 mL | Baxter | 1001936040 | |
| Nanozoomer Digital Pathology system | Hamamatsu | ||
| IgM ELISA Quantification Kit | Bethyl Laboratories | E90-101 |
Referências
- Hyde, D. M., Hamid, Q., Irvin, C. G. Anatomy, pathology, and physiology of the tracheobronchial tree: emphasis on the distal airways. J Allergy Clin Immunol. 124, S72-S77 (2009).
- Rosenthal, N., Brown, S. The mouse ascending: perspectives for human-disease models. Nat Cell Biol. 9, 993-999 (2007).
- Peters, L. L., et al. The mouse as a model for human biology: a resource guide for complex trait analysis. Nat Rev Genet. 8, 58-69 (2007).
- Baron, R. M., Choi, A. J., Owen, C. A., Choi, A. M. Genetically manipulated mouse models of lung disease: potential and pitfalls. Am J Physiol Lung Cell Mol Physiol. 302, 485-497 (2012).
- Sharma, S. Acute respiratory distress syndrome. BMJ Clin Evid. 2010, (2010).
- Saguil, A., Fargo, M. Acute respiratory distress syndrome: diagnosis and management. Am Fam Physician. 85, 352-358 (2012).
- Wilson, M. S., Wynn, T. A. Pulmonary fibrosis: pathogenesis, etiology and regulation. Mucosal Immunol. 2, 103-121 (2009).
- Wuyts, W. A., et al. The pathogenesis of pulmonary fibrosis: a moving target. Eur Respir J. 41, 1207-1218 (2013).
- Mouratis, M. A., Aidinis, V. Modeling pulmonary fibrosis with bleomycin. Curr Opin Pulm Med. 17, 355-361 (2011).
- Moeller, A., Ask, K., Warburton, D., Gauldie, J., Kolb, M. The bleomycin animal model: a useful tool to investigate treatment options for idiopathic pulmonary fibrosis?. Int J Biochem Cell Biol. 40, 362-382 (2008).
- Myllärniemi, M., Kaarteenaho, R. Pharmacological treatment of idiopathic pulmonary fibrosis – preclinical and clinical studies of pirfenidone, nintedanib, and N-acetylcysteine. European Clinical Respiratory Journal. 2, (2015).
- Reinert, T., Baldotto, C. S. d. R., Nunes, F. A. P., Scheliga, A. A. d. S. Bleomycin-Induced Lung Injury. Journal of Cancer Research. 2013, 1-9 (2013).
- Lakatos, H. F., et al. Oropharyngeal aspiration of a silica suspension produces a superior model of silicosis in the mouse when compared to intratracheal instillation. Exp Lung Res. 32, 181-199 (2006).
- Helms, M. N., Torres-Gonzalez, E., Goodson, P., Rojas, M. Direct tracheal instillation of solutes into mouse lung. J Vis Exp. , (2010).
- Osier, M., Oberdorster, G. Intratracheal inhalation vs intratracheal instillation: differences in particle effects. Fundam Appl Toxicol. 40, 220-227 (1997).
- Driscoll, K. E., et al. Intratracheal instillation as an exposure technique for the evaluation of respiratory tract toxicity: Uses and Limitations. Toxicol Sci. 55, 24-35 (2000).
- MacDonald, K. D., Chang, H. Y., Mitzner, W. An improved simple method of mouse lung intubation. J Appl Physiol (1985). 106, 984-987 (1985).
- Spoelstra, E. N., et al. A novel and simple method for endotracheal intubation of mice. Lab Anim. 41, 128-135 (2007).
- Cai, Y., Kimura, S. Noninvasive intratracheal intubation to study the pathology and physiology of mouse lung. J Vis Exp. , e50601 (2013).
- Starcher, B., WIlliams, I. A method for intratracheal instillation of endotoxin into the lungs of mice. Lab Anim. 23, 234-240 (1989).
- Daubeuf, F., Frossard, N. Performing bronchoalveolar lavage in the mouse. Curr Protoc Mouse Biol. 2, 167-175 (2012).
- Li, Y., et al. Severe lung fibrosis requires an invasive fibroblast phenotype regulated by hyaluronan and CD44. J Exp Med. 208, 1459-1471 (2011).
- Grazioli, S., et al. CYR61 (CCN1) overexpression induces lung injury in mice. Am J Physiol Lung Cell Mol Physiol. 308, L759-L765 (2015).
- Redente, E. F., et al. Tumor necrosis factor-alpha accelerates the resolution of established pulmonary fibrosis in mice by targeting profibrotic lung macrophages. Am J Respir Cell Mol Biol. 50, 825-837 (2014).
- Lawrenz, M. B., Fodah, R. A., Gutierrez, M. G., Warawa, J. Intubation-mediated intratracheal (IMIT) instillation: a noninvasive, lung-specific delivery system. J Vis Exp. , e52261 (2014).
