Procedures involving animal subjects have been approved by the Dutch Central Committee for Animal Experiments and the Animal Care Committee at University Medical Center Groningen (NL). Both Wistar and Lewis rats with weights between 180 and 300 g were used.
1. Housing and Acclimatization
- After arrival at the central animal facility, house rats in groups of 5 per cage. During a 7-day acclimatization period, accustom the rats to human handling, but do not perform any experimental procedures.
2. Preparation and Injection of Sterile Monocrotalin
- For 1 mL of 60 mg/mL monocrotalin (MCT) solution, weigh 60 mg of monocrotalin in a 2-mL tube. Add 700 µL of 0.9% NaCl. Add 200 µL of 1 M HCl. Warm the solution in the tube under hot running tap water and vortex it. Use 6 N NaOH to bring the pH towards 7.0. Use sterile technique for preparation of MCT for injection into rodents.
- Inject 1 mL of sterile 60 mg/mL MCT solution per kg subcutaneously in the neck (0.3 mL of 60 mg/mL MCT for a 300-g rat). NOTE: We prefer not to use smaller volumes due to the greater chance that the injected dose will not be appropriate.
3. Aorta-caval Shunt Surgery
- Anesthesia.
- Fill the induction chamber with 5% isoflurane/100% O2 (flow: 1 L/min) and place the rat in the chamber. Check for adequate depth of the anesthesia by performing a hind toe pinch. Weigh the rat.
- Shave and clean the abdomen over an area that is approximately 8 cm long and 3 cm wide. Place the rat on its back on a heat mat (37 °C) covered by a sterile mat.
- Place the snout in a ventilation mask/hood with 2 – 3% isoflurane/100% O2 (flow: 1 L/min). Check the depth of anesthesia by performing a hind toe pinch. Apply eye ointment to prevent dryness while under anesthesia.
- Shunt Surgery.
- Scrub the skin with chloride-hexidine for disinfection. Inject 0.01 mg/kg buprenorphine subcutaneously for post-operative analgesia.
- Use sterile instruments for surgery. Make an incision with a #10 scalpel blade in the abdomen on the midline, starting 1 cm below the diaphragm an extending down to just above the genitalia.
- Lift up the intestine with a cotton swab, cover the intestines in a sterile, wet gauze (0.9% NaCl), and place them to the left side of the animal.
- Use cotton swabs to separate the membranes that attach the abdominal aorta and the vena cava inferior to the surrounding tissues.
NOTE: Do not dissect the membranes between the aorta and the vena cava. - Using splinter forceps, remove the perivascular aortic fat just above the bifurcation, only on the right side of the aorta and only on the site where the needle will be inserted.
- Use cotton swabs to separate the aorta and vena cava from 2 mm superior to the site where the needle will be inserted in order to create space for a Biemer clamp.
- At this area, first place a loose ligature (5-0 suture) around the aorta. Create tension on the ligature by placing a Kocher clamp on it, and then place the Kocher superior to the incision (Figure 1A). Place the Biemer clamp just superior to the ligature (Figure 1A).
- Using a cotton swab, compress the vena cava as distally as possible to obstruct the flow (Figure 1A). Bend a needle (18 G in this protocol) into a 45-degree angle, with the orifice pointing towards the outside (Figure 1A).
- At an angle of 90 degrees, insert the needle in the aorta, just above the bifurcation, with the orifice of the needle pointing to the left (Figure 1A). Manipulate the tip of the needle to the left and insert it into the vena cava.
NOTE: The needle tip should now be visible in the vena cava (Figure 1B). - Use a second cotton swab to push the remaining blood in the aorta out of the insertion site to prevent thrombosis. Dry the area around the shunt with a sterile gauze in order for the glue to adequately stick.
- Pull the entire needle out of the aorta and immediately apply a drop of tissue glue onto the puncture site in the aorta. Make sure not to glue the cotton swab to the tissue. Unclamp the aorta.
- Verify the shunt manually by pulling on and releasing the ligature on the aorta proximal to the shunt. Loosening should color the vena cava distal to the shunt in bright red and create turbulence at the shunt site.
NOTE: Tightening will turn the blood in the vena cava back to dark red. - Place the intestines back in the animal. Close the muscle layer and skin with resorbable 4-0 sutures. Ventilate the animal with 100% O2 to recover from anesthesia.
NOTE: Do not leave an animal unattended until it has regained sufficient consciousness to maintain sternal recumbency.
- Sham Surgery.
- Perform all of the above procedures except for the insertion of the needle into the aorta.
- Post-surgical care.
- Place the rat in a single cage and into an incubator at 37 °C until the next morning.
- Around 6 h after surgery, inject 0.01 mg/kg buprenorphine subcutaneously for post-operative analgesia. Repeat the next morning if the rat shows signs of discomfort.
NOTE: The first 3 days after surgery, rats tend to eat and drink less (this is particularly important when chow or drinking water are mixed with drugs). Most rats show normal behavior 3 days after surgery. If not, monitor closely. Weight loss exceeding 15% in 1 week is considered abnormal, and such rats should be euthanized by the extraction of the circulating blood volume while under anesthesia.
4. Development of PAH
NOTE: In this protocol, the animal is euthanized by the extraction of the circulating blood volume while under anesthesia.
- Sacrifice 1 day after the surgery (MF8) for the early cellular and functional responses to increased pulmonary blood flow (e.g., gene up-regulation or early transcription factors).
- Sacrifice 1 week after the surgery (MF14) for an early-stage PAH vascular phenotype (medial hypertrophy without neointimal lesions).
- Sacrifice 2 weeks after the surgery (MF21) for an advanced-stage PAH vascular phenotype (marked medial hypertrophy and neointimal formation) with mild elevation in RVP and mPAP.
- Sacrifice 3 weeks after the surgery (MF28) for an end-stage PAH vascular phenotype (marked neointimal occlusion) and strong elevation in RVP and mPAP. Clinical signs of right ventricular failure are common in this stage.
- Sacrifice after day 28 (MF-RVF) for PAH-associated right ventricular failure (RVF), clinically defined as dyspnea, severe lethargy, and weight loss (< 10% in 1 week). Terminate rats when one of these signs is present. Frequently, rats develop these symptoms between days 28 and 35 and, if left unguarded, die spontaneously during this time interval.
5. Right Heart Catheterization
- Anesthesia.
- Fill the induction chamber with 5% isoflurane/100% O2 (flow: 1 L/min) and place the rat in the box. Check for adequate depth of the anesthesia by performing a hind toe pinch. Weigh the rat.
- Shave and clean the neck at the right-ventral side of the rat and, for the echocardiography protocol, the thorax and upper abdomen.
- Place the rat on its back on a heat mat (37 °C) and place the snout in a ventilation mask/hood with 2 – 3% isoflurane/100% O2 (flow: 1 L/min). The snout should be faced towards the researcher.
- Check depth of anesthesia. Be careful with rats with severe PH. If the heart rate decreases, reduce the depth of anesthesia. Preferable, perform all measurements within 20 min. Apply eye ointment to prevent dryness while under anesthesia.
- Echocardiography protocol.
- Perform the echocardiography according to the protocol described by Brittain et al. in JoVE13.
- Catheterization protocol.
NOTE: This protocol uses a rigid cannula with a preformed tip bent 20 degrees to guide the 15-cm silicon catheter with a ball 2 mm from the tip. A 20-G needle with its orifice slightly bent to the inside is used to insert the cannula into the right jugular vein (see the list of materials). Rats in any phase of PAH progression and control can be used in this protocol.- Disinfect the neck with chloride-hexidine. Make a 1.5-cm incision with a #10 scalpel blade in the right-ventral side of the neck, from the right collar bone to the mandibular bone.
- Spread the tissue using scissors. Using tweezers, gently pull the tissue apart until the jugular vein appears. Dissect the membranes around the jugular vein using splinter forceps.
- Put tension on the jugular vein by placing a loose ligature (5-0 suture) around the vessel. Increase the tension and tape the ligature onto the ventilation mask (Figure 2A).
- Downstream of the insertion site, place a loose ligature around the vessel to tighten after the cannula is in situ in order to prevent leakage and loss of pressure.
- Using the handles of a forceps, slightly bend the tip of a 20-G needle with the orifice to the inside to conduct the cannula with the catheter.
- Introduce the tip of the 20-G needle into the vein and quickly place the cannula containing the catheter inside the vessel. Pull out the needle, and then close the ligature that was prepared in step 5.3.4.
- Conduct the cannula containing the catheter into the jugular vein. The tip of the cannula is at a 20-degree curve (see step 5.3.5). Maneuver the cannula under the collar bone and advance a little to enter the right atrium (Figure 2C).
- To enter the right ventricle, point the tip of the cannula to the left, towards the heart (Figure 2D). On the bedside monitor, an RV pressure curve should appear, matching Figure 2D.
- When the RV pressure curve is constant, write down the systolic and diastolic right ventricular pressure 1 (sRVP1/dRVP1).
- Manipulate the tip of the cannula to the left and upwards. Advance the catheter within the cannula (Figure 2E).
- Advance the catheter into the main pulmonary artery (PA). No resistance should be felt when passing the pulmonary valve.
NOTE: When the catheter enters the main pulmonary artery, the diastolic pressure will rise. On the bedside monitor, a PA pressure curve should appear, matching Figure 2E. - When the PA pressure curve is constant, write down the systolic, diastolic, and mean PA pressure 1 (sPAP1, dPAP1, mPAP1).
- Further advance the catheter within the cannula until the ball at the tip of the catheter gets wedged in a pulmonary artery. Observe the pressure curve on the bedside monitor drop and match the wedge pressure curve in Figure 2F.
- When the wedge pressure curve is constant, write down the systolic, diastolic, and mean wedge pressure.
- Pull back the catheter slowly and subsequently measure and write down the values for sPAP2, dPAP2, mPAP2, sRVP2, and dRVP2, as displayed on the bedside monitor.
- When in the RV, slightly pull back the cannula and catheter to measure the mean right atrial pressure (RAP). The curve should match the RAP curve in Figure 2A.
NOTE: In this protocol, the rats are euthanized after the catheterization protocol by the extraction of the circulating blood volume while under anesthesia.
6. Morphology Assessment and Morphometry
NOTE: In this protocol, the animal is euthanized by the extraction of the circulating blood volume while under anesthesia. Rats in any phase of PAH progression and control can be used in this protocol.
- After sacrifice, take out the lungs by cutting the trachea about 5 mm above the bronchial bifurcation and the vessels that connect the lungs to the heart. Put the lungs in cold saline. Dissect the left lung. Cut the left main bronchus at the bifurcation.
- Fill a 50-mL syringe with 4% paraformaldehyde, attach a tube with a cannula to the syringe, and hang the syringe about a meter above the work table. Fit the cannula in the left main bronchus to passively fill the lung with paraformaldehyde. Handle paraformaldehyde with caution.
- Incubate the left lung in paraformaldehyde for 48 h.
- Dehydrate the left lung by incubating it consecutively in 70% ethanol (1 h), 80% ethanol (1 h), 90% ethanol (1 h), 100% ethanol (3 h), xylol (2 h), and paraffin (2 h).
- Embed the left lung in paraffin, with the hilum of the lung facing the cassette.
- Stain the paraffin-embedded, 4-µm lung sections using a Verhoeff or Elastica-van Gieson staining, as per manufacturer's instructions29. Make sure the elastic laminae are well differentiated (as in Figure 3). Scan the stained sections at 40X magnification.
- Divide the lung into 4 quadrants. In each quadrant, find 10 vessels with an outer diameter < 50 µm (intra-acinar) and 10 vessels with an outer diameter > 50 µm (pre-acinar). Take a picture (2 x 40 pictures per lung). Zoom in randomly up to 20x magnification and photograph every vessel in this field of view to minimize selection bias.
- Exclude vessels that have a longest/shortest diameter ratio of > 2, an incomplete circular shape, or a collapse of more than one quarter of the vessel wall.
NOTE: An example of an excluded vessel is shown in Figure 3b Make each picture on the same magnification (40X) and include a scale bar. - Open ImageJ and the first picture. Draw a straight line on the scale bar in the picture to set the scale via "Analyse" and "Set scale." For "known distance," use the value on the picture's scale bar. Use micrometers (µm) as the unit of length. Set the scale to global.
- Using "freehand selections," draw a line on the inner border of the luminal area (Figure 3), and use "measure" (crtl m) to measure this area. Then, draw a line around the outer elastic lamina (Figure 3) to measure the total vessel area.
- Calculate the luminal and outer diameter (
 ) using
) using  .
. - Calculate wall thickness using
 .
. - Calculate the wall/lumen ratio using
 .
. - Calculate the occlusion score using
 .
. - Score the vessel on muscularization (no, partial, or total muscularization) (Figure 3B).
NOTE: Vessels with a double elastic lamina for more than half the circumference are defined as totally muscularized. Vessels with a double elastic lamina less than half the circumference are defined as partially muscularized. - Score the vessel on the presence of a neointima (yes or no) (Figure 3C).
NOTE: Vessels without a clearly-defined internal elastic lamina combined with (often eccentric) luminal occlusion are defined as neointimal lesions.
Representative results are presented in Figure 4. The presented results show characteristics of MCT+FLOW in Lewis rats in the following groups: Control (n = 3), MF8 (n = 5), MF14 (n = 5), MF28 (n = 5), and MF-RVF (n = 10). Statistical analyses were performed using the one-way ANOVA with Bonferroni correction.
60 mg/kg MCT and increased pulmonary blood flow lead to a mean rise in systolic right ventricular pressure (sRVP) (23 ± 6 to 56 ± 11 mmHg), systolic pulmonary artery pressure (sPAP) (20 ± 4 to 54.0 ± 10 mmHg), and mean pulmonary artery pressure (mPAP) (16 ± 3 to 36 ± 4 mmHg) at 28 days (MF28). They remain equally high up to the stage when right ventricular failure develops (MF-RVF) (Figure 4). At the early PAH stages (MF8 and MF14), no rise in sRVP, sPAP, and mPAP is observed. Diastolic PAP and right atrial pressure increase in the late phases, but not significantly. Wedge pressures do not change significantly during disease progression.
The right ventricular-to-left ventricular and septal weight ratio increases significantly from MF14 to MF-RVF, indicating right ventricular hypertrophy. The liver's wet-to-dry weight ratio is significantly increased at the MF-RVF stage, indicating liver edema and congestive right ventricular failure.
Muscularization of intra-acinar vessels < 50 µm increases progressively during PAH progression. Vessels of this size normally do not have a muscular medial layer in control rats. At MF14, almost half of these vessels (43 ± 17%) has a total muscular media (as in Figure 3B). At MF28 and MF-RVF, nearly every arteriole is muscularized (98.7 ± 2.5% and 100 ± 0%). Neointimal lesions first occur at MF21, while at MF28 and MF-RVF, around 65% of all arterioles have a neointimal layer (as in Figure 3C). The arteriolar wall-to-lumen ratio and occlusion scores both increase significantly from MF14 to MF28 (respectively, 10.4 ± 3.9 to 71.5 ± 30 (con: 7.1 ± 0.2) and 20.0 ± 2.8 to 54.7 ± 10.6 (con: 12.2 ± 0.3)). The hemodynamic and histomorphological characteristics of PAH progression in MCT+FLOW in Wistar rats are similar14.
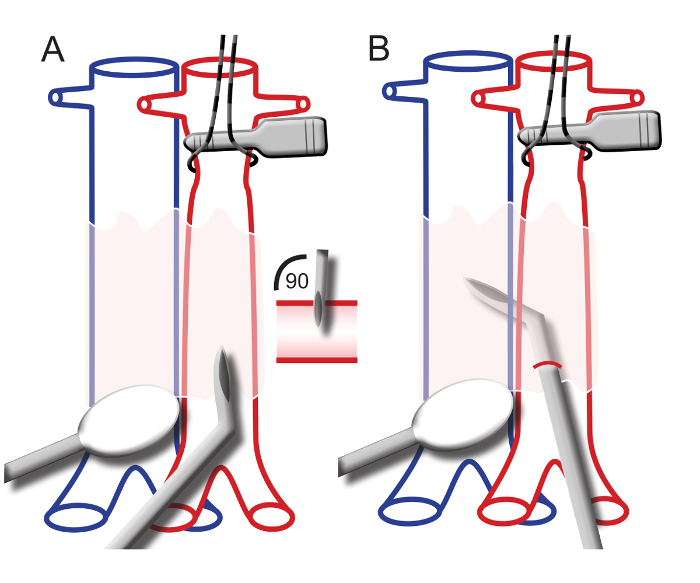
Figure 1. Schematic Representation of the Aorto-caval Shunt Surgery. A) The aorta is tensioned and clamped superior to the insertion site. The vena cava is compressed inferior to the insertion site. The needle, bent at 45° and with the orifice to the outside, is inserted into the aorta at a 90° angle. B) The needle is positioned in the aorta with the tip inserted into the vena cava. Please click here to view a larger version of this figure.
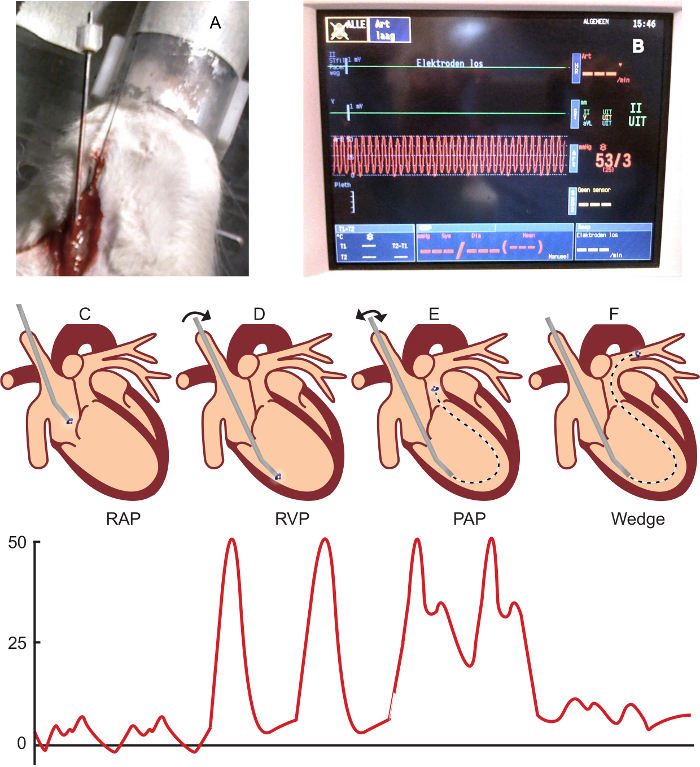
Figure 2. Right Heart Catheterization Procedure and Representative Pressure Curves. A) The right jugular vein is tensioned with a ligature and taped onto the ventilation mask. The catheter is placed into the jugular vein. B) A bedside monitor displaying a right ventricular pressure wave. C) The catheter within the cannula placed in the right atrium after introduction into the right jugular vein. Below: a typical right atrial pressure wave. D) The catheter within the cannula placed in the right ventricle. Below: a typical right ventricular pressure wave in end-stage PAH. E) The catheter is advanced in the cannula to enter the main pulmonary artery. Below: a typical pulmonary arterial pressure wave. F) The catheter is advanced into the pulmonary arteries until a wedge pressure wave is displayed on the monitor. Below: a typical pulmonary wedge pressure wave. Please click here to view a larger version of this figure.
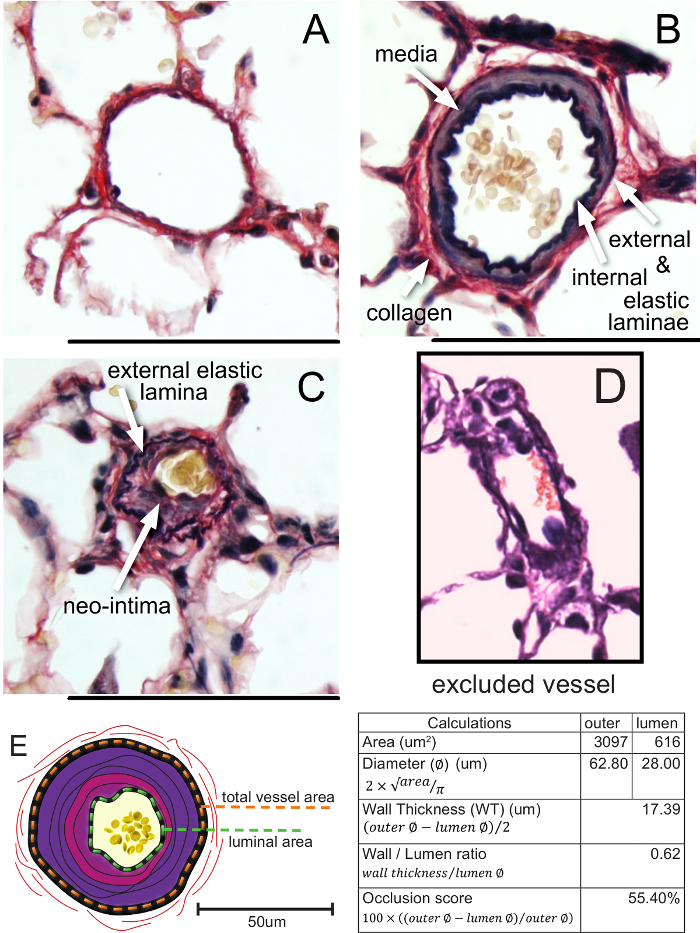
Figure 3. Vascular Morphology and Morphometry in Control and PAH Rats. A) A normal, non-muscularized vessel with an occlusion score of 3.7%. B) A totally muscularized arteriole with an occlusion score of 24.3%. C). A neointimal lesion with an occlusion score of 54.1%. D) An excluded vessel (longest/shortest diameter ratio of > 2 and an incomplete circular shape). E) The measurement of the total vessel and luminal area (in a vessel with a schematic representation of a neointimal lesion), including calculations. The bars represent 50 µm. Please click here to view a larger version of this figure.
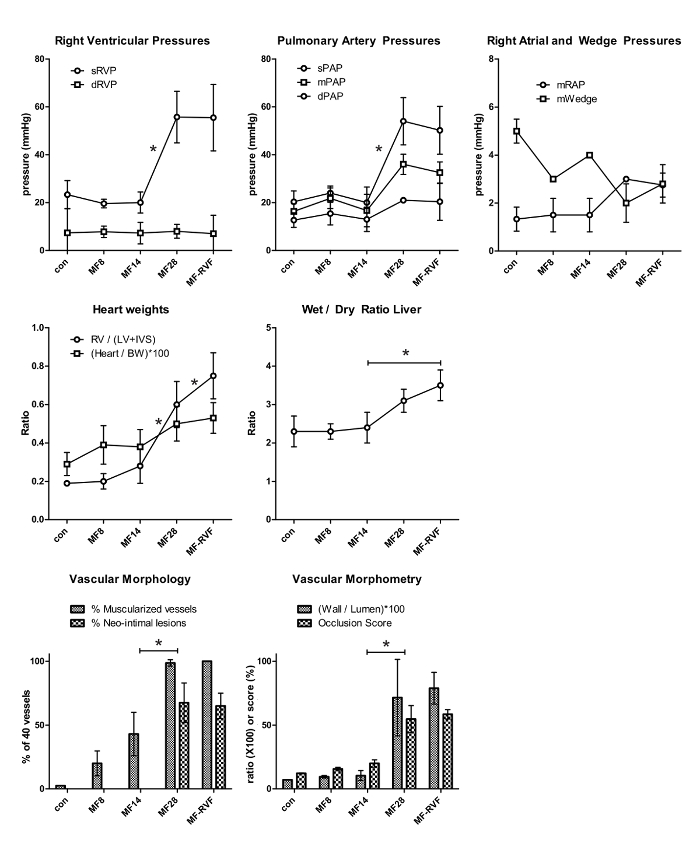
Figure 4. Representative Results of Pulmonary Hemodynamics and Vascular Morphology/Morphometry. The statistical analyses were performed using the one-way ANOVA with Bonferroni corrections. Values are represented as the mean ± SEM. con: control; MF (monocrotalin + flow); RVF: right ventricular failure; s: systolic; d: diastolic; m: mean; RVP: right ventricular pressure; PAP: pulmonary arterial pressure; RAP: right atrial pressure. RV: right ventricle; LV: left ventricle; IVS: interventricular septum; BW: body weight. Please click here to view a larger version of this figure.
