Intraductal Delivery to the Rabbit Mammary Gland
Summary
Here, we describe a technique for the localized delivery of reagents to the rabbit mammary gland via an intraductal injection. In addition, we describe a protocol for visualization and the confirmation of delivery by high-resolution ultrasound imaging of contrast agents.
Abstract
Localized intraductal treatments for breast cancer offer potential advantages, including efficient delivery to the tumor and reduced systemic toxicity and adverse effects1,2,3,4,5,6,7. However, several challenges remain before these treatments can be applied more widely. The development and validation of intraductal therapeutics in an appropriate animal model facilitate the development of intraductal therapeutic strategies for patients. While the mouse mammary gland has been widely used as a model system of mammary development and tumorigenesis, the anatomy is distinct from the human gland. A larger animal model, such as the rabbit, may serve as a better model for mammary gland structure and intraductal therapeutic development. In contrast to mice, in which ten ductal trees are spatially distributed along the body axis, each terminating in a separate teat, the rabbit mammary gland more closely resembles the human gland, with multiple overlapping ductal systems that exit through separate openings in one teat. Here, we present minimally invasive methods for the delivery of reagents directly into the rabbit mammary duct and for visualization of the delivery itself with high-resolution ultrasound imaging.
Introduction
The intraductal delivery of therapeutic agents has been studied in rodent models and in early stage human trials3,4,5,6,11,12. A recent Phase I study demonstrated the safety and feasibility of intraductal carboplatin or intraductal pegylated liposomal doxorubicin in women awaiting mastectomy for the treatment of invasive cancer2.
Previous protocols for intraductal delivery have been developed for mouse and rat mammary glands6,7,8,9. For research purposes, intraductal tumor cell injections and the lentiviral vector delivery of oncogenes have also been performed in rodent models13,14,15,16. However, an ideal in vivo model of the intraductal delivery process should permit the development of novel classes of therapeutic compounds and facilitate preclinical assessment. Anatomical differences between rodents and humans have complicated the translation of these studies.
Unlike mice, in which each duct ends at a separate teat, the human breast consists of 5 to 9 independent ductal systems, each with a separate opening ending at the teat. Rabbit mammary glands harbor four independent ductal systems, each separately accessible through one of four orifices in a single teat. A rabbit model more closely matches the human anatomy and permits the study of intraductal drug delivery in a more relevant context.
Here, we use two techniques to assess intraductal delivery. The co-administration of a vital dye permits visualization through the skin and provides a simple and rapid confirmation of the method. For some applications, higher resolution mapping of the ducts may be preferred. We present here a protocol for ultrasound imaging of the ducts through the intraductal delivery of a non-targeted contrast reagent.
Protocol
Procedures using animal subjects have been approved by the Institutional Animal Care and Use Committee of the University of Texas at Austin.
1. Preoperative Preparation
- Record the body weight of each rabbit. As with all preclinical studies, monitor animal weights regularly to assess potential toxicity.
- Prior to anesthetizing the rabbit, fill a 50 mL conical tube with commercially available ultrasound gel and spin at 500 x g for 30 s; there should be no visible bubbles in the gel upon completion of the centrifugation.
- Administer glycopyrrolate subcutaneously at a dose of 0.1 mg/kg and acepromazine intramuscularly at a dose of 0.75 mg/kg. Wait 15-20 min for the sedative to take effect while monitoring vital signs and behavior.
NOTE: Glycopyrrolate is an anti-cholinergic agent that prevents bradycardia and reduces respiratory and GI secretions. Acepromazine is a sedative that serves as a premedication for anesthesia. - Administer 35 mg/kg of ketamine and 5 mg/kg of xylazine subcutaneously as an anesthetic. However, as the operator becomes more experienced and can accomplish the intraductal delivery more rapidly, decrease the drug dosages to 15 mg/kg of ketamine and 3 mg/kg of xylazine subcutaneously; this will shorten the anesthesia time and the time required for the animal to recover from anesthesia.
- Check and document the heart rate, SPO2, temperature, respiratory rate, and mucus membrane color every 15 min. Apply eye lubricant to both eyes.
NOTE: Only personnel who have undergone appropriate training and have been approved by their institution's IACUC should administer or monitor anesthesia. The use of a veterinary anesthesia monitor can aid in acquiring vital signs and is recommended. The veterinary anesthesia monitor, however, does not replace the need to manually check the animal every 15 min. See the manufacturer's instructions for the proper use of a veterinary monitor. - Verify the onset of anesthesia by a gentle toe pinch; the rabbit should be non-responsive before continuing.
- Carefully shave the caudal abdomen of the rabbit in the area around the third and fourth pairs of inguinal teats.
- With the majority of the hair removed, apply an over-the-counter hair removal cream to the shaved area. Remove the cream 10 min after application using damp paper towels wetted with warm water.
NOTE: Rabbit skin is very fragile/sensitive. The hair removal cream should be used for no more than 10 min. In fact, it is safer to try a “test spot” at 5 min and only leave on longer if test spot indicates a longer time period is needed. - Wipe the area with alcohol-soaked gauze pads to clean the injection site.
- Place the rabbit on its dorsum in a v-shaped trough lined with a recirculating warm water blanket and an absorbent pad.
2. Preparation of the Contrast Agent
- Reconstitute the non-targeted contrast reagent according to the manufacturer's instructions. Pipette up and down gently to mix.
NOTE: The contrast agent used in this protocol is stable at room temperature for 4 – 6 h after reconstitution. Gently rock the vial between each retrieval.
NOTE: The volume of solution required will depend on the number of ducts to be injected. The rabbit has 4 ductal openings per teat, and 0.2 mL of solution is sufficient to fill one ductal tree of an adult New Zealand White Rabbit (Oryctolaguscuniculus). Thus, a total volume of 0.8 mL may be delivered to one mammary gland.
3. Intraductal Delivery
- Locate the appropriate teats to be injected; the 3rd and 4th pairs of inguinal teats are recommended, as they are easily visualized when the animal is positioned on its dorsum.
- Load 0.2 mL of sterile 0.9% saline into a 1 mL Luer-lock tuberculin syringe with a 22 G needle. Properly dispose of the 22 G needle once the saline is in the syringe and replace it with a sterile 25-gauge needle. Gently wipe the area with 85% isopropyl alcohol on a gauze pad.
- With the bevel of the needle up and the syringe parallel to the body of the animal, insert the bevel of the needle into the side of the teat and slowly inject 0.1-0.2 mL of saline; this will allow for better visualization of the ductal openings.
- Load 0.2 mL of injection solution into a 1 mL Luer-lock tuberculin syringe.
- Hold the teat gently with the thumb and index finger and lift it slightly to position it for the intraductal injection; a wearable ocular loupe may aid in visualizing the ductal openings.
- While maintaining the lifted position of the teat, carefully cannulate the duct of interest using a 25 G blunt-tip needle.
- After cannulation, gently twist the Luer-lock syringe on the hub of the blunt-tip infusion needle until it is locked in place.
- Lift the teat and inject the solution slowly to minimize potential damage caused by rapidly moving fluid within the duct; at no time should there be resistance when injecting the solution.
4. Ultrasound Imaging
- Apply a liberal amount of centrifuged ultrasound gel to the skin of the area of interest. Ensure that there are no bubbles in the gel, as these will compromise the image quality.
- Set the imaging depth to 6 mm. Place the 21-MHz transducer in contact with the gel and scan the area of interest in B-mode. Observe the contrast medium in the scanned region including the ductal opening and throughout the duct.
NOTE: These settings have been developed for use with a specific photoacoustic ultrasound machine. Refer to the Table of Materials for more details. It may be necessary to adjust the transmit power and imaging depth of other imaging systems to optimize mammary gland visualization. - Remove the ultrasound gel from the animal's skin with a gauze pad.
5. Postoperative Care
- Observe the injection site: there should be no signs of trauma to the teat region or to the surrounding tissue, and swelling in the area surrounding the teat likely indicates a mammary fat pad injection rather than a successful intraductal injection.
- Place the rabbit in a sternal position. If needed, give 0.2 mg/kg of yohimbine intravenously to the marginal ear vein; this will reverse the effect of the xylazine and allow the animal to recover more quickly from anesthesia.
- Monitor the rabbit every 15 min throughout the recovery period until the animal is alert, responsive, and maintains a sternal position.
NOTE: This procedure should not result in tissue damage or swelling. If redness or swelling are observed, administer a dose of meloxicam 0.1-0.2 mg/kg PO once the animal is alert and able to take medication orally. Contact the institution's veterinary staff for further guidance.
Representative Results
Here, we show that the intraductal delivery of contrast reagents to the mammary ducts of a rabbit can be achieved without trauma to the tissue (Figure 2). In rabbits, four separate ductal systems converge at one teat and thus may be accessed and imaged individually using this method. Individual ductal openings are easily visualized; note the arrowhead marking a second ductal opening adjacent to the cannulated duct in Figure 2B.
High-resolution ultrasound imaging with untargeted contrast reagent in linear imaging mode can provide a real-time readout of the intraductal delivery. Representative images show detection of the reagent up to 45 min post-delivery (Figure 3). This technique may also be useful for monitoring the kinetics of therapeutic delivery through the ducts.
The robustness of this injection method is highly dependent upon the operator. To master the injection technique, it is recommended to inject a solution of 0.2% Evans Blue dye and monitor the integrity of the gland. This provides the operator with an additional readout of success and also aids in the determination of the appropriate volumes to be injected into each gland. Simple visual assessment can be used to determine whether the dye reaches the entire ductal system (Figure 4) and whether any ducts are damaged during the delivery.
Figure 1: Schematic of Rabbit Mammary Glands. The two lower pairs of dots represent the teats of the inguinal glands. Please click here to view a larger version of this figure.
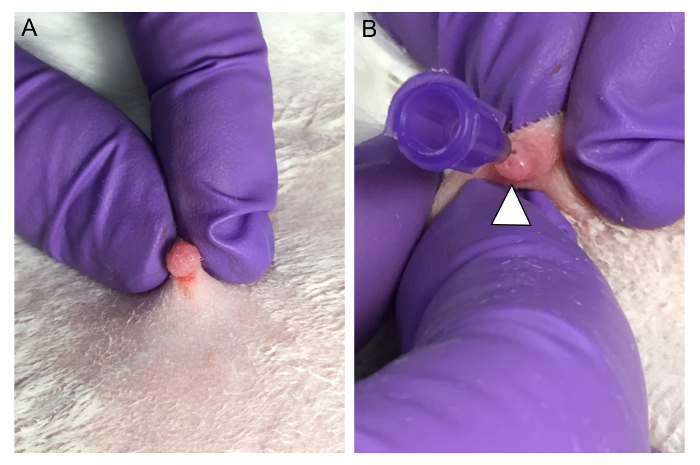
Figure 2: Preparation and Cannulation of the Inguinal Mammary Gland for Intraductal Delivery. (A) The teat of the right inguinal mammary gland is shown here immediately after the delivery of 0.2 mL of 0.9% sterile saline. Upon injection, the ductal openings are visualized more clearly. (B) A ductal opening in the same teat is then cannulated with a 25 G blunt-tip infusion needle. The arrow shows a ductal opening without a cannula. Please click here to view a larger version of this figure.
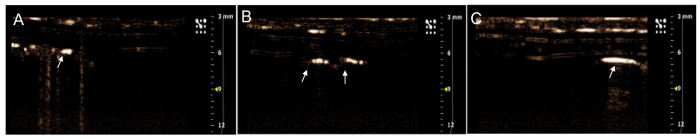
Figure 3. Non-targeted Contrast Reagent Visualized within the Mammary Duct by Ultrasound Imaging. (A) The contrast reagent is localized immediately after delivery and is visualized (B) 30 min post-delivery and (C) 45 min post-delivery. The persistence of the reagent inside the mammary duct allows visualization throughout the duration of this protocol. Please click here to view a larger version of this figure.
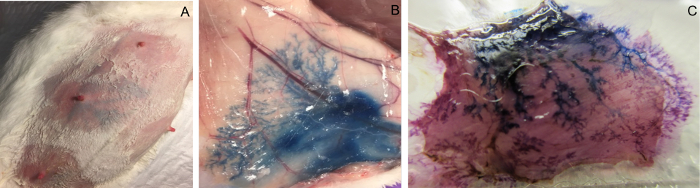
Figure 4: An Inguinal Mammary Gland Injected through the Teat with Evans Blue Saline Solution. (A) The external appearance after the intraductal injection of 0.2 mL of Evans Blue solution. (B) Upon opening the skin, the Evans Blue permits the visualization of the entire mammary ductal tree and confirms the intact ductal structure. (C) Whole-mount specimen of a region of inguinal mammary gland after fixation and staining with carmine alum. Please click here to view a larger version of this figure.
Discussion
This method of intraductal delivery to the rabbit mammary gland may be used for ultrasound contrast reagents and many other aqueous solutions, including vital dyes and therapeutics. Previous studies have demonstrated the intraductal delivery of hormones17,18,19. In rodent models, the intraductal delivery of nucleic acids8, chemotherapeutics6,7, and nanoparticle carriers8,20 have been performed. The protocol described here could be adapted for these applications as well.
For some applications, the confirmation of the intraductal delivery by Evans Blue vital dye, as visualized through the skin, may be sufficient. However, visualization through the skin is diffuse, and individual ducts are not well demarcated. In endpoint studies, Evans Blue vital dye does provide a clear map of the entire ductal tree, but this requires the isolation of the mammary tissue. Therefore, contrast-enhanced ultrasound provides an alternative approach for visualizing the intraductal delivery to individual ducts in live animal studies. We note that Evans Blue dye maps the entire ductal tree, including the smallest-diameter terminal ducts, while contrast reagent and ultrasound maps only include the larger ducts. Another distinction is the possibility to monitor temporal dynamics in ultrasound, whereas Evans Blue provides only a single snapshot measurement.
As in the method for intraductal delivery to the rodent mammary duct9, the most significant challenge and limitation to this technique is likely to be the reliance on operator expertise. However, the larger size of the ductal openings in a rabbit model simplifies the procedure, eliminates the need for performing the technique with the aid of a stereomicroscope, and shortens the time required for new operators to develop proficiency. In our experience, the injection of 0.1-0.2 mL of saline to the side of the teat prior to the intraductal delivery is a critical step that enables the clear visualization of the ductal openings (step 3.2, above). Accurate positioning and lifting of the delivery site is also essential; this ensures that the solution flows into the duct (steps 3.5 and 3.6, above). We note that the co-administration of the contrast reagent will necessarily reduce the available volume for testing other reagents or therapeutics. However, intraductal delivery can also be performed without imaging or with simple inspection by Evans Blue to confirm the delivery.
The most common noninvasive lesion of the breast is ductal carcinoma in situ (DCIS), in which abnormal ductal epithelial cells proliferate inside the mammary duct but do not penetrate through the basement membrane to the adjacent tissue. With advances in mammographic imaging, the detection rates of DCIS have increased dramatically. In the United States, approximately 25% of newly diagnosed breast lesions are classified as DCIS, and by 2020, more than 1 million women will be living with DCIS in the United States alone22,23,24,25. However, many DCIS lesions remain dormant, and most estimates find that only 15-40%21,22,23,24,25 of DCIS lesions will ever progress to invasive cancer. However, there are currently no predictive biomarkers to aid in the identification of which tumors will become invasive.
As more women are diagnosed with this pre-cancerous lesion, serious questions regarding over-diagnosis and overtreatment have emerged. The treatment of premalignant disease is typically aggressive. Most patients with DCIS will undergo surgery (lumpectomy or mastectomy), and many also receive radiation25. Some patients with hormone receptor-positive DCIS will also receive 5 or more years of endocrine therapy, which has been shown to reduce recurrence. Side effects of this treatment may include stroke, blood clots, bone loss, and elevated risks of uterine and endometrial cancers. All of these options have serious systemic side effects and impact patient quality of life. There is a significant need for less invasive therapeutic strategies25.
The intraductal delivery of chemotherapeutic agents in both mouse models and in breast cancer patients has previously been shown to be effective, with no evidence of systemic toxicity or long-term histopathological changes3,4,5,6. The intraductal administration of therapeutics could one day offer new options for women diagnosed with DCIS that has not yet progressed to a locally invasive lesion. The potential for halting tumorigenesis while also preserving ductal structure makes this an attractive therapeutic strategy10. Importantly, the localized delivery approach ensures that the treatment reaches the relevant abnormal cells while potentially minimizing collateral damage to other tissues. While rabbit tumor models are not available, the normal mammary gland of rabbits may provide a relevant model to test the localized delivery, safety, transport, and kinetics of therapeutics uptake inside the mammary duct. These in vivo studies will enable the testing and validation of candidate diagnostics and therapeutics within a relevant tissue environment.
A similar approach enabled the intraductal administration of therapeutics to live mice and allowed for minimally invasive and localized drug delivery to the mammary ductal system8,9. However, the anatomy of the mouse mammary gland differs from the human breast in a number of important ways, including the tissue composition and the number of ducts that end at each teat. Here, we extend this technique to a larger animal model in which the mammary epithelial structure more closely represents the anatomy of the human breast12,14. This opens up the possibility for extended monitoring by imaging and for assaying the concomitant intraductal delivery of various reagents to the rabbit mammary ductal epithelium. Advances in localized delivery to an appropriate animal model, with ductal anatomy similar to the human gland, should accelerate the application of non-invasive, targeted therapeutic strategies in humans.
Declarações
The authors have nothing to disclose.
Acknowledgements
The authors acknowledge support from a Translational Breast Cancer Research Grant (14-60-26-BROC to AB) from the Breast Cancer Research Foundation and the American Association for Cancer Research.
Materials
| MicroMarker non-targeted contrast reagent | VisualSonics | VS-11694 | |
| Luer Lock 1mL Syringes | BD | 309628 | |
| Glycopyrrolate 0.2mg/mL | Wedgewood Compounding Pharmacy | GLYCOP-INJ013VC | 6 month shelf life, supply may be limited. |
| Atropine Sulfate 0.5 mg/mL | Animal Health International | 15320764 | If glycopyrrolate is unavailable. Not to be combined with glycopyrrolate. |
| Ketamine HCL 100mg/mL | Animal Health International | 21250699 | http://www.animalhealthinternational.com/ |
| Acepromazine 10mg/mL | Animal Health International | 17640541 | |
| Xylazine 20mg/mL | Animal Health International | 20101547 | |
| Yohimbine 0.2mg/mL | Animal Health International | 14588965 | |
| Hair Removing Cream | Veet | Sensitive skin solution. Available through local retailers. | |
| Blunt tip infusion needles | Sai Infusion Technology | B14-50 | http://www.sai-infusion.com/collections/blunt-needles |
| Veterinary Pulse Oximeter | EdanUSA | VE-H100B | http://www.edanusa.com/Product/VE-H100B-Veterinary-Pulse-Oximeter.html |
| Warm Water Pump | Gaymar | TP700 | |
| Warm Water Blanket | Animal Health International | 21232696 | Maxi-Therm Lite Warming Pads |
| Ultrasound system | VisualSonics | Vevo 2100 |
Referências
- Flanagan, M., Love, S., Hwang, E. S. Status of Intraductal Therapy for Ductal Carcinoma in Situ. Curr Breast Cancer Rep. 2 (2), 75-82 (2010).
- Love, S. M., et al. A Feasibility Study of the Intraductal Administration of Chemotherapy. Cancer Prevention Research. 6 (1), 51-58 (2013).
- Stearns, V., et al. Preclinical and Clinical Evaluation of Intraductally Administered Agents in Early Breast Cancer. Sci Transl Med. 3 (106), 106ra108 (2011).
- Zhang, B., et al. The Safety Parameters of the Study on Intraductal Cytotoxic Agent Delivery to the Breast before Mastectomy. Chin J Cancer Res. 26 (5), 579-587 (2014).
- Mahoney, M. E., Gordon, E. J., Rao, J. Y., Jin, Y., Hylton, N., Love, S. M. Intraductal Therapy of Ductal Carcinoma In Situ: a Presurgery Study. Clin Breast Cancer. 13 (4), 280-286 (2013).
- Murata, S., et al. Ductal Access for Prevention and Therapy of Mammary Tumors. Cancer Res. 66 (2), 638-645 (2006).
- Chun, Y. S., et al. Intraductally Administered Pegylated Liposomal Doxorubicin Reduces Mammary Stem Cell Function In the Mammary Gland but in the Long Term, Induces Malignant Tumors. Breast Cancer Res Treat. 135 (1), 201-208 (2012).
- Brock, A., et al. Silencing HoxA1 by Intraductal Injection of siRNA Lipidoid Nanoparticles Prevents Mammary Tumor Progression in Mice. Sci Trans Med. 6 (217), 2172a2 (2014).
- Krause, S., Brock, A., Ingber, D. E. Intraductal Injection For Localized Drug Delivery To The Mouse Mammary Epithelium. J Vis Exp. (80), e50692 (2013).
- Brock, A., Goh, H. T., Yang, B., Yu, L., Li, H., Loh, Y. H. Cellular Reprogramming: A New Technology Frontier In Pharmaceutical Research. Pharm Res. 29 (1), 35-52 (2012).
- Silverstein, M. J., et al. Ductal Carcinoma In Situ of the Breast. Annu. Rev Med. 51, 17-32 (2000).
- Love, S. M., Barsky, S. H. Anatomy of the Nipple And Breast Ducts Revisited. Cancer. 101 (9), 1947-1957 (2004).
- Virnig, B. A., Shamliyan, T., Tuttle, T. M., Kane, R. L., Wilt, W. J. Diagnosis and Management of Ductal Carcinoma In Situ (DCIS). Evidence Report/Technology Assessment. , 185 (2009).
- Mills, D., et al. Examination of Duct Physiology in the Human Mammary Gland. PLoS One. 11 (4), e0150653 (2016).
- King, B. L., Love, S. M. The Intraductal Approach to the Breast: Raison d’Etre. Breast Cancer Res. 8 (2), 206 (2006).
- Bu, W., Xin, L., Toneff, M., Li, L., Li, Y. Lentivirus vectors for stably introducing genes into mammary epithelial cells in vivo . J Mammary Gland Biol Neoplasia. 14, 401-404 (2009).
- Lyons, W. R. The Direct Mammotrophic Action of Lactogenic Hormone. Proc. Soc. Exp. Bio. Med. 51 (2), 308-311 (1942).
- Fiddler, T. J., Birkinshaw, M., Falconer, I. R. Effects Of Intraductal Prolactin On Some Aspects of the Ultrastructure and Biochemistry of Mammary Tissue in the Pseudopregnant Rabbit. J Endocrinol. 49 (3), 459-469 (1971).
- Falconer, I. R., Fiddler, T. J. Effects of Intraductal Administration Of Prolactin, Actinomycin D and Cycloheximide on Lipoprotein Lipase Activity in the Mammary Glands of Pseudopregnant Rabbits. Biochim Biophys Acta. 218 (3), 508-514 (1970).
- Singh, Y. Influence of Molecular Size on the Retention of Polymeric Nanocarrier Diagnostic Agents in Breast Ducts. Pharm Res. 29 (9), 2377-2388 (2012).
- Jain, R., et al. Atypical Ductal Hyperplasia: Interobserver and Intraobserver Variability. Mod Pathol. 24 (7), 917-923 (2011).
- Betsill, W. L., Rosen, P. P., Lieberman, P. H., Robbins, G. F. Intraductal Carcinoma. Long-term Follow-up After Treatment by Biopsy Alone. JAMA. 239 (18), 1863-1867 (1978).
- Eusebi, V., et al. Long-term Follow-up of In Situ Carcinoma of the Breast. Semin Diagn Pathol. 11 (3), 223-235 (1994).
- Sanders, M., et al. The Natural History Of Low-Grade Ductal Carcinoma In Situ Of The Breast In Women Treated By Biopsy Only Revealed Over 30 Years Of Long-Term Follow-Up. Cancer. 103 (12), 2481-2484 (2005).
- Esserman, L. J., et al. Addressing Overdiagnosis and Overtreatment in Cancer: A Prescription For Change. Lancet Oncol. 15 (6), e234-e242 (2014).
