Baseline Characteristics of the Airway Immune Profiles:
Complete data on upper airway mucosal immune mediator levels at 1 month of age was obtained in 620 (89%) of the 700 children enrolled in the COPSAC2010 cohort. Ten neonates were enrolled before the technique was established, and 19 did not attend the 1-month visit. Additionally, 47 samples were excluded because they were extracted and measured in another laboratory used in a pilot study, and 4 samples were lost in transportation (See the study flowchart, Figure 1). Baseline characteristics for the cohort are shown in Table 1.
Most of the mediators had a low level of detection <10 pg/mL (IL-1β, IL-2, IL-4, IL-5, IL-10, IL-12p70, IL-13, IL-17A, TGF-β1, IFN-γ, TNF-α, CXCL8, CCL13, CCL4, and CCL17), whereas 5 had a detection level >10 pg/mL (CXCL10, CCL2, CCL11, CCL26, and CCL22) (Table 2). The median (IQR) number of samples below the detection limit (i.e. from 0 to the lower limit of detection) for each mediator was 29 (7.25 – 119.5) (Table 2). IFN-γ levels were below the lower detection limit in almost half (46%) of the samples, whereas CXCL8 and IL-1β levels were detectable in all samples, and TGF-β1, CCL4, and TNF-α levels were below the lower detection limit in <1% of the samples. One of the mediators, TSLP, was only detected in 2% of samples, and TSLP data was therefore not used for consecutive data analyses. A strong multicollinearity was evident for the 20 detected immune mediator levels, which is visualized in a heatmap (Figure 2).
The Influence of Airway Bacteria and Viruses in Neonates:
We previously found an association between the airway immune profile and colonization in specific airway bacteria sampled concomitantly with mucosal lining fluid at 1 month of age. An upregulated Type 1- and Type 17-based airway immune profile was observed in neonates colonized with intracellular bacteria, whereas the presence of extracellular bacteria was associated with a Type 17-based profile7. We have also shown previously that the presence of picornavirus was associated with an upregulated profile comprised mainly of Type 1 immune mediators (Figure 3)11. These findings were obtained in children without respiratory symptoms, (i.e. asymptomatic) on the day of sampling, suggesting an immune-triggering role of colonizing bacteria and viruses in the earliest part of life.
The Influence of Pre- and Perinatal Exposure:
We have further observed an association between the level of immune mediators at 1 month of age and a maternal history of atopy8, where children born to atopic mothers displayed an overall lower level of immune mediators than children of non-atopic mothers. We subsequently identified an association between the presence of siblings in the household at birth and a specific Type 1/Type 17-directed mucosal immune response, with evidence of this being related to an in utero immune priming effect, as the immune response was inversely correlated to the time since last childbirth (Figure 4)12. Further evidence for in utero immune priming effects was determined from an association between maternal H1N1 influenza vaccination status and the upregulation of TGF-β1 levels in the neonatal airway10.
Evidence for Micronutrient Mechanisms of Action:
In COPSAC2010, we performed a high-dose versus standard-dose vitamin D intervention trial during pregnancy, which showed an almost one-fourth reduction in the risk of asthma/recurrent wheeze in the offspring at 3 years of age9. Utilizing the measured neonatal airway immune profile, we observed that children born to mothers receiving high-dose vitamin D, compared to standard-dose, were characterized by an upregulation of specific mediators (IL-12p70, IL-13, CCL17, TGF-β1, and IL-2), suggesting that vitamin D promotes an anti-bacterial defense system different from that induced by bacteria, virus, siblings, and maternal atopy9 (Figure 5).
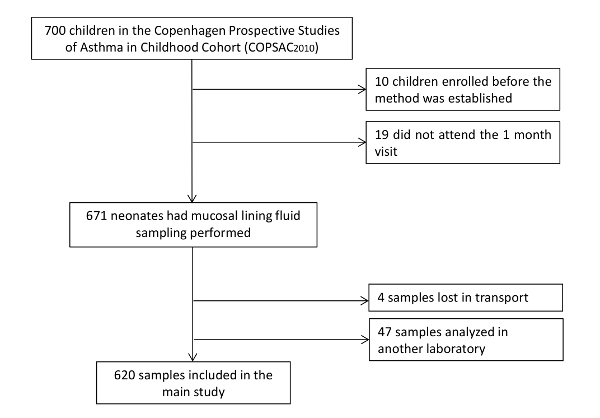
Figure 1: Study Group Flowchart. Complete data on upper airway mucosal immune mediator levels at 1 month of age was obtained in 620 (89%) of the 700 children enrolled in the COPSAC2010 cohort. Ten neonates were enrolled before the technique was established, and 19 did not attend the 1-month visit. Additionally, 47 samples were excluded because they were extracted and measured in another laboratory used in a pilot study, and 4 samples were lost in transportation. Please click here to view a larger version of this figure.
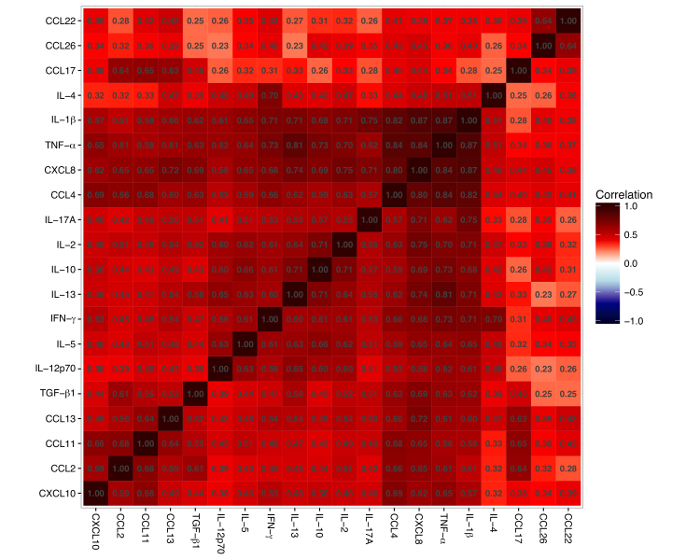
Figure 2: Heatmap of Pairwise Correlations between the 20 Cytokines and Chemokines. The red color represents a positive correlation and the blue color represents a negative correlation. The number inside every square denotes the correlation between two mediators. The figure shows that all mediators are positively correlated. Please click here to view a larger version of this figure.
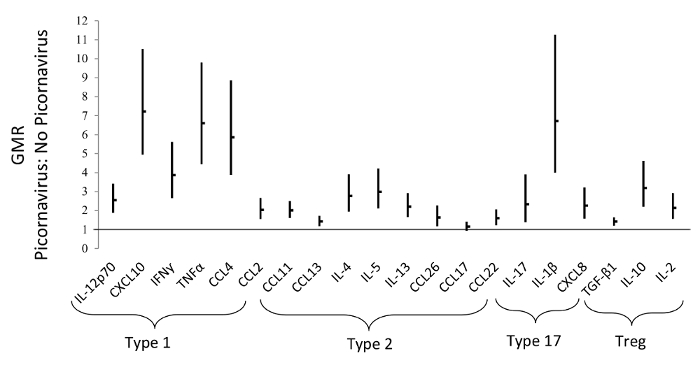
Figure 3: The Presence of Picornavirus is Associated with an Upregulated Profile Comprised Mainly of Type 1 Immune-mediators. This figures shows the Geometric Mean Ratios (GMR), with 95% Confidence Intervals (CI), of airway mediators in neonates with/without the concomitant presence of picornavirus, measured at 1 month of age. This figure has been modified from Wolsk et al.11, with permission. Please click here to view a larger version of this figure.
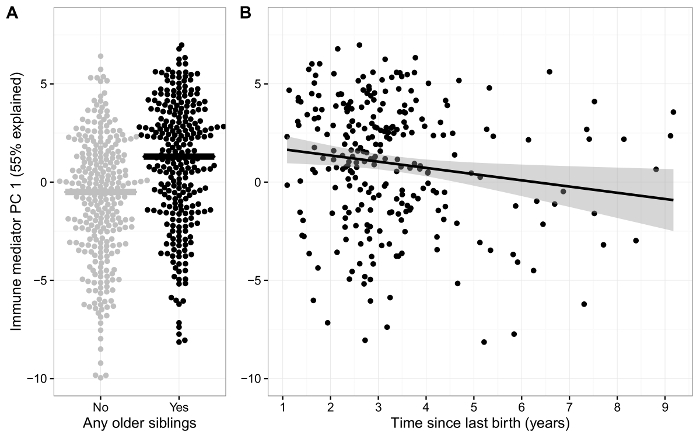
Figure 4: Effects of the Presence of Siblings in the Household at Birth. A) Airway immune signature (PC1) in neonates with and without siblings at birth. B) Scatterplot showing an inverse association between the airway immune signature (PC1) and time since previous birth for children with siblings. This figure has been modified from Wolsk et al.12, with permission. Please click here to view a larger version of this figure.
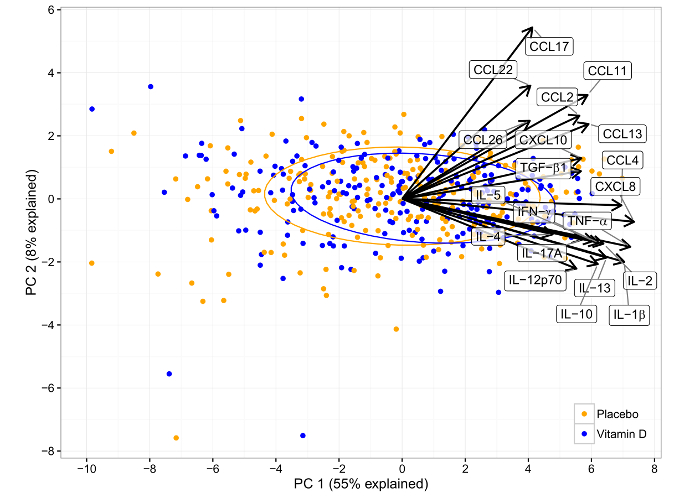
Figure 5: Principal Component Analysis Biplot of the Effect of Vitamin D Intervention in the COPSAC2010 Cohort on the Airway Immune Mediator Level at 1 Month of Age. Each point represents a sample, colored according to the intervention allocation of the child. The loadings (i.e. impact) of the original variables on the principal components are shown as arrows. The intervention resulted in a significantly upregulated immune profile in PC1, which is positively correlated with all immune mediators. This figure has been modified from Chawes et al.9, with permission. Please click here to view a larger version of this figure.
| N = 620 (%) | |
| Maternal atopy | 334 (54) |
| Non Caucasian | 29 (5) |
| Cesarean section | 134 (22) |
| Antibiotics in 3rd trimester | 126 (20) |
| Siblings in the home at birth | 358 (58) |
| Pets (cat and/or dog) in the home | 216 (35) |
| Fully-breastfed at 1 month | 570 (92) |
| No smoking in 3rd trimester | 597 (96) |
| No alcohol consumption in 3rd trimester | 591 (95) |
| Family income >100.000 euro/year | 89 (14) |
| Gestational age >37 weeks | 601 (97) |
| Apgar score >7 at 5 min | 591 (95) |
Table 1: Baseline Characteristics of the COPSAC2010 Cohort.
| Mediator | Detection limit pg/ml | < Detection limit N (%) | Median pg/ml | IQR pg/ml |
| IL-12p70 | 1.4 | 102 (16%) | 10.80 | 4.99 – 22.22 |
| CXCL10 | 31 | 8 (1%) | 1787.78 | 722.8 – 5423 |
| IFN-γ | 4.1 | 285 (46%) | 20.14 | 7.63 – 48.51 |
| TNF-α | 0.6 | 5 (<1%) | 28.33 | 10.06 – 88.55 |
| CCL4 | 4.3 | 4 (<1%) | 194.90 | 71.22 – 655.8 |
| CCL2 | 16.0 | 9 (1%) | 256.11 | 134.4 – 468.5 |
| CCL13 | 2.8 | 13 (2%) | 15.17 | 10.35 – 22.80 |
| IL-4 | 1.1 | 196 (32%) | 1.37 | 0.42 – 2.86 |
| IL-5 | 1.2 | 172 (28%) | 3.72 | 1.42 – 8.10 |
| IL-13 | 2.7 | 48 (8%) | 14.49 | 6.84 – 27.51 |
| CCL11 | 22.0 | 39 (6%) | 139.54 | 85.00 – 236.0 |
| CCL26 | 45.0 | 252 (41%) | 164.93 | 56.33 – 350.02 |
| CCL17 | 7.2 | 90 (15%) | 41.30 | 26.83 – 60.68 |
| CCL22 | 25.0 | 78 (13%) | 398.31 | 243.4 – 575.7 |
| IL-1β | 0.4 | 0 (0%) | 225.49 | 50.07 – 1169 |
| IL-17A | 1.5 | 285 (46%) | 1,480 | 0.43 – 4.79 |
| CXCL8 | 3 | 0 (0%) | 19465 | 6321 – 38274 |
| TGF-β1 | 5.2 | 1 (<1%) | 28.66 | 20.76 – 39.50 |
| IL-10 | 1 | 13 (2%) | 22.32 | 9.28 – 49.16 |
| IL-2 | 1.5 | 19 (3%) | 18.72 | 8.29 – 37.33 |
Table 2: Mucosal Lining Fluid Samples from 1-month-old Neonates from the COPSAC2010 Cohort. Most of the mediators had a low level of detection <10 pg/mL (IL-1β, IL-2, IL-4, IL-5, IL-10, IL-12p70, IL-13, IL-17A, TGF-β1, IFN-γ, TNF-α, CXCL8, CCL13, CCL4, and CCL17), whereas 5 had a detection level >10 pg/mL (CXCL10, CCL2, CCL11, CCL26, and CCL22).
