Rat Model of the Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy (ALPPS) Procedure
Summary
Inducing rapid liver hypertrophy using Associating Liver Partition and Portal vein ligation for a Staged hepatectomy (ALPPS) has been proposed for resection of borderline resectable liver tumors. This model may elucidate mechanisms involved in rapid hypertrophy and allows testing of drugs that promote or block the acceleration of regeneration.
Abstract
Recent clinical data support an aggressive surgical approach to both primary and metastatic liver tumors. For some indications, like colorectal liver metastases, the amount of liver tissue left behind after liver resection has become the main limiting factor of resectability of large or multiple liver tumors. A minimal amount of functional tissue is required to avoid the severe complication of post-hepatectomy liver failure, which has high morbidity and mortality. Inducing liver growth of the prospective remnant prior to resection has become more established in liver surgery, either in the form of portal vein embolization by interventional radiologists or in the form of portal vein ligation several weeks prior to resection. Recently, it was shown that liver regeneration is more extensive and rapid, when the parenchymal transection is added to portal vein ligation in a first stage and then, after only one week of waiting, resection performed in a second stage (Associating Liver Partition and Portal vein ligation for Staged hepatectomy = ALPPS). ALPPS has rapidly become popular across the world, but has been criticized for its high perioperative mortality. The mechanism of accelerated and extensive growth induced by this procedure has not been well understood. Animal models have been developed to explore both the physiological and molecular mechanisms of accelerated liver regeneration in ALPPS. This protocol presents a rat model that allows mechanistic exploration of accelerated regeneration.
Introduction
The size of the liver remnant limits the resectability of liver tumors.1 In general, when less than 25% liver tissue is left behind, the patient is at increased risk of death from acute liver failure due to the lack of metabolic function for the entire organism ("too small for size syndrome").2 This post-hepatectomy liver failure is the most devastating complication after liver resection. Therefore clinicians have tried to induce liver regeneration prior to resection of the liver by manipulating the flow of the portal vein.3 It was found that, once the portal vein is occluded, the remaining part with portal vein flow starts to grow at a slow rate, and can thereby increase up to 60% in size.4 Surgical ligation5 or interventional portal vein occlusion have both been clinically established.4 The increase in volume and function of the liver is reliable, but the growth rate of the liver after portal occlusion is only about one fifth compared to the growth of the remnant liver after partial hepatectomy.6
The time necessary for the liver to grow is weeks to months even though the liver can regenerate at a much faster rate after resection. As such, the liver is the only organ that grows back to normal function after removal of a part of it.7 A novel procedure inducing liver regeneration at a similar pace as after partial hepactectomy was developed by a group of surgeons who discovered that adding a transection between the occluded and the non-occluded part of the liver induces liver hypertrophy at the same growth rate as after liver resection, but prior to resection.9 The procedure initiates rapid hypertrophy of 80% within a week in the future liver remnant, which allows the resection of extensive, primarily unresectable, liver tumors within a week. The procedure was called "Associating Liver Partition and Portal vein ligation for Staged hepatectomy = ALPPS" and became rapidly popular across the world.10 Multiple reports supported an expansion of the resectability of borderline resectable liver tumors achieved by the new technique,11 while the complex surgical procedure was also criticized for its high complication rate.12,13
The development of a rodent and also large animal models of slow and rapid hypertrophy has been attempted since the publication of ALPPS in 2012 to allow a better histological characterization and understanding of the mechanisms and to test drug effects on the different growth rates of liver tissue in animals. The first animal model developed was a rat model. In this model, rapid hypertrophy after parenchymal transection between the right and the left part of the median lobe accelerated regeneration of the right median lobe.14 A different model was introduced later in the mouse. In this model the left lateral lobe was resected and the portal vein branches to every lobe of the liver except the left median lobe were tied.15 In the meantime, large animal models of ALPPS in pigs have been described as well.16
For the study of physiological mechanisms like flow changes and pressure in the portal vein, perfusion and oxygenation of liver tissue, the rat model is superior to the model of ALPPS in mice. Another advantage of the rat over the murine model is that in the rat model there is no necessity for a resection of the left lateral lobe,15 which may contaminate the effects of liver resection with those of ALPPS. The rat model in contrast does not reduce the liver cell mass. A pig model uses the right posterior lobe as the growing lobe, but the pig liver is highly lobulated. Therefore, it is difficult to create a transection plane in the already thin tissue bridge between the right posterior and the right anterior lobe. In contrast, the median lobe in rats consist of two parts that are separately supplied by a portal vein each and a parenchymal transection plane can easily be created between the two using microsurgical techniques. The availability of small animal computer tomography (CT) and/or magnet resonance imaging (MRI) allows the very exact quantification of volumetric growth between portal vein ligation alone and portal vein ligation and the added transection, which is important for the validation of any rapid liver hypertrophy model.
The protocol presented here describes the surgical technique and procedures used for volumetric validation and physiological characterization of the model of slow and rapid hypertrophy after portal vein ligation and portal vein ligation with transection, respectively, in rats.
Protocol
All experiments in this protocol were approved by the Veterinary Authorities of the Canton of Zürich, Switzerland (number 60/2014). Furthermore, all experimental steps were performed in strict compliance with the Guidelines on Experiments with Animals by the Swiss Academy of Medical Sciences (SAMS) and Guidelines of the Federation of European Laboratory Animal Science Associations (FELASA).
1. Animal Husbandry, Operating Room Equipment and Instruments, Anesthesia
- Keep male Wistar rats with a weight of 250-300 g in ventilated cages under standard pathogen-free conditions in a 12/12 h light/dark cycle. Give animals free access to food and water at an ambient temperature of 22 ± 1 °C.
- Induce anesthesia in a box, where isoflurane is flushed in with 5 vol% for 30 s (Figure 1A), followed by an isoflurane concentration of 3 vol% until the animal is under deep anesthesia. Confirm the level of anesthesia by the toe-pinch reflex.
- Provide analgesia using subcutaneously applied buprenorphine (0.01 mg/kg) during the surgical intervention, followed by 0.02 mg/kg every 12 h in the postoperative phase for 48 h.
- Transfer the animal to the working place, where they are spontaneously breathing exposed to a gas mixture of 1.0 – 2.5 vol% isoflurane in oxygen (flow: 600 mL/min).
- Close the eyes of the animal and use an ointment to protect the eyes. Inject 5 mL saline subcutaneously, half of it on each side of the abdomen, followed by 0.1 mg atropine.
- Perform surgery using a surgical microscope in a microsurgery room.
- Keep the animal under volatile anesthesia using a ventilation mask consisting of a latex membrane (Figure 1B), through which the rat's snout is pushed. Fix the extremities with tape (Figure 1B).
- Lay out the surgical instruments in sterile fashion on a side table: saline- and Betadine-soaked sponges (Figure 2A), abdominal wall retractors (Figure 2B) as well as 3-0 sutures for retraction of the abdominal wall and xiphoid, scissors, Adson forceps, fine tips microforceps straight and curved and pre-cut 6-0 silk ties for the ligation procedure (Figure 2C).
- Use non-sticking bipolar microforceps for transection of the hepatic parenchyma. Close the abdominal wall and skin using 3-0 silk sutures with SH-1 needles and 5-0 Maxon (Figure 2D). Use a bipolar forceps for hemostasis.
2. Start of Surgery
- Shave the abdomen of the animal with a small animal hair clipper from the xiphoid to the genitals with a 2-cm area lateral of the midline. Thoroughly remove the hair.
- Disinfect this area 3 times with betadine soaked sponges.
- Perform a midline incision using a scalpel for the skin, and then use surgical scissors to open the abdomen.
- Retract the right and left abdominal wall and the xiphoid with 3-0 silk sutures (Figure 3A).
- Retract the stomach, colon and small bowel from the hepatoduodenal ligament of the rat with self-made small wire retractors (Figure 3B).
3. Portal Vein Ligation (PVL)
- Access the portal vein and its branches by lateral retraction of the stomach and the small bowel (Figure 3B).
- Dissect the portal vein bluntly by picking up the peritoneum with the microforceps and slowly peeling it medially.
- Dissect the portal vein branches out (Figure 3C) in the following sequence: (1) right posterior branch, (2) left lateral and left median branch together, and (3) caudate branch.
- First, peel off the peritoneum with small, not too energetic moves to avoid tearing the small arterial branches to the liver lobes that run directly under the peritoneal coverage.
- Once the main portal vein is denuded, encircle the branches with slow forward pushing and spreading movements and then pull a 1-cm piece of 6-0 silk tie around the respective portal vein branch and ligate it.
- Ligate the right posterior lobe branch. (Figure 3C) The technical difficulty of the right posterior branch consists in the fact that the artery to the right posterior lobe is running across the right posterior portal vein branch.
- Pull the artery cranially together with the peritoneum to expose the right portal vein branch with the curved microforceps.
- Ligate the right posterior lobe branch with the pre-cut 6-0 silk tie. The right posterior lobe turns visibly pale once the portal vein is ligated.
- Avoid pushing against resistance during the circling to prevent tearing the artery or the portal vein. In case of bleeding, apply pressure for at least one minute with a sterile cotton swab and then reassess. If bleeding does not stop, sacrifice the animal.
- Ligate the left lateral (LLL) and left median lobe (LML) branches. These branches have one common trunk. (Figure 3C). The left median lobe branch arises from the portal vein within the parenchyma of the LLL.
- Ligate the portal vein leading to both LLL and also the LML branch together using the pre-cut 6-0 silk tie.
- Avoid injuries to the arteries leading to LLL and LML, running within the peritoneal layer. As long as the peritoneum is peeled back carefully, they stay intact. The LLL and LML turn visibly pale once the branches are ligated.
- Ligate the caudate lobe branch (Figure 3C). The portal vein leading to the somewhat separate caudate lobes in rats takes off from the main portal vein, distally and medially to the takeoff of the right lobe branch from the main portal vein (not strictly inferiorly like in humans or larger animals).
- Dissect it out and encircle it by lifting up the peritoneum plus bile duct and arteries from the main portal vein.
- Encircle the caudate portal vein branch with a curved microforceps coming from laterally. The two caudate lobes turn visibly pale, once the caudate lobe branch is ligated with 6-0 silk.
- Tying these three portal vein branches leads to exclusive portal vein perfusion of the right median lobe (RML), which is visible by a distinct demarcation line between the right and left median lobe.
4. Portal Vein Ligation with Transection (PVL+T)
- Perform the transection along the demarcation line between RML and LML after PVL (Figure 3D).
- Use a non-sticking bipolar silver forceps with a very fine neurosurgical tip to precauterize the liver tissue creating a 1-mm cauterization strip along the demarcation line.
- Use scissors to carefully cut the precauterized tissue. It is quite difficult to properly assess the depth of the transection. The goal is to get as close to the vena cava as possible, which runs intrahepatically in rats. Injury of the vena cava is accompanied by extensive bleeding, which can usually not be stopped.
- In case of injury apply gentle pressure using a cotton-swab, but if the bleeding does not stop within 3 – 4 min, sacrifice the animal. Attempts at repairing the vena cava using sutures have generally been unsuccessful. Rats are very sensitive to air embolism, which may occur on occasion and lead to cardiac arrest.
5. Intraoperative Measurement of Portal Vein Pressure and Volume Flow
- Assess portal vein pressure by direct cannulation with a G30 needle connected to a pressure monitor (Figure 4A).
- Use the 2-mm volume flow probe placed laterally connected to the flow device for direct measurement of portal volume flow over 2 min (Figure 4B). Only record data with stable measurement quality as indicated on the machine display.
- Assess portal vein flow and pressure separately after the group of steps that define the respective procedure, i.e. the tying off of three portal vein branches or the tying off of the three portal vein branches plus performing the parenchymal transection between the RML and the LML.
6. Final Steps of Surgery
- Make sure that the small bowel is placed properly in the abdominal cavity before closing.
- Close the peritoneum and the abdominal wall with 3-0 silk sutures with SH-1 needles.
- Finally suture the skin using Maxon 5-0.
- Disinfect the skin again.
- Apply again 5 mL saline subcutaneously into the subcutaneous tissue lateral to the abdomen.
7. Liver Volumetry in Rats Using Small Animal CT
- 24 h prior to the first CT imaging inject 200 μL of the contrast agent into the tail vein through a G26 intravenous catheter.
- Use a micro CT to scan the rats. Place the animal in a plexiglas box to induce general anesthesia (first flush in with 5 vol% for 30 s, followed by an isoflurane concentration of 2 – 3 vol% until the animal is under anesthesia and maintain it throughout scanning via a tubing system). For optimal image quality, synchronize the CT scan with the respiration of the animal.
- Export the digital imaging and communications in medicine (DICOM) files and analyze them using the public domain imaging platform OsiriX 8.0. Use the "closed polygon" tool to draw the lobe borders based on the radiodensitiy of the nanoparticle contrast in the liver and use the region of interest (ROI) menu to calculate partial liver volumes (see Figure 2A in Schadde et al.17)
- In the standard model, allow the liver to grow over 3 days and obtain daily CT scans to assess volume increase.
Representative Results
The two different surgical procedures portal vein ligation (PVL) and PVL with transection (PVL+T) result in distinctly different growth kinetics. PVL induces moderate volume increase within 3 days, whereas in PVL+T a much larger right median lobe (RML) can be seen (Figure 5). This can be verified by daily volumetry. The volume of the RML roughly doubles within 3 days in PVL, while it triples in PVL+T.17
Flow measurements in the portal vein reveal a stable flow, despite the reduced flow area in the PLV and also the PVL+T (see Figure 3A in Schadde et al.17). This suggests that the entire portal blood volume flow is directed through approximately 26% of the previous liver parenchyma, thereby causing "portal hyperflow".
Pressure measurement inside the portal vein reveals an acute increase of the mean portal vein pressure from 5 mmHg to 9 mmHg in PVL and PVL+T (see Figure 3B in Schadde et al.17). This is likely a result of the portal hyperflow. Transection alone does not result in an acute portal pressure increase, since the volume of liver tissue is not reduced.17 Repeated measurements show that the pressure increase remains stable for 24 h.17
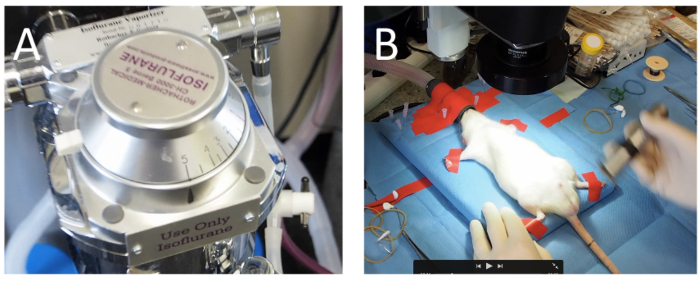
Figure 1: Anesthesia. (A) After flushing a box with isoflurane (5 vol%) to induce anesthesia for the animal, isoflurane is vaporized (600 mL oxygen/min) for maintenance of general anesthesia. (B) The animals are fixated on a sterile operating surface under an operating microscope. Please click here to view a larger version of this figure.
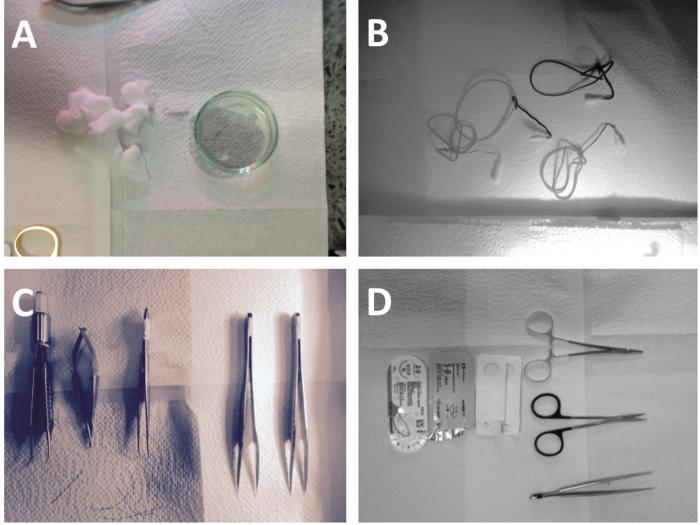
Figure 2: Sterile Equipment. (A) Sterile moist sponges for exposure and retraction. (B) Wire mini-tractors connected to rubber bands. (C) Bipolar forceps, Potts scissors; curved microforceps, straight microdissectors are used for dissection of the portal vein branches. (D) Larger scissors, needle holders and needles are used for opening and closure. Please click here to view a larger version of this figure.
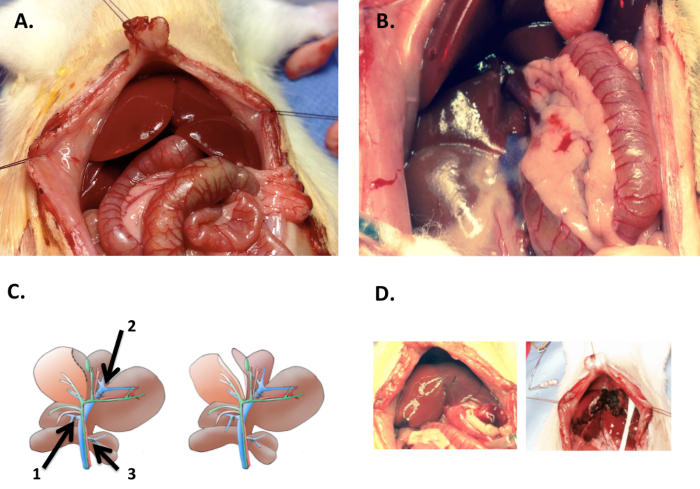
Figure 3: Dissection. (A) The sides of the abdomen and the xiphoid are retracted with 3-0 silk sutures after midline laparotomy. (B) By retracting the stomach, small and large bowel laterally the gastroduodenal ligament in rats and the hepatic hilum can be exposed. (C) In portal vein ligation (PVL), the portal vein branch to the right lobes (1), the left lateral lobe (2) and the caudate lobes (3) are ligated with 6-0 silk ties (left). In PVL with transection (PVL+T), additionally, the ischemic demarcation line between right median lobe (RML) and left median lobe (LML) is transected (right). (D) The photograph shows the distinct demarcation line between LML and RML (left). This line is followed for the transection using a bipolar microforceps for PVL+T (right). Please click here to view a larger version of this figure.
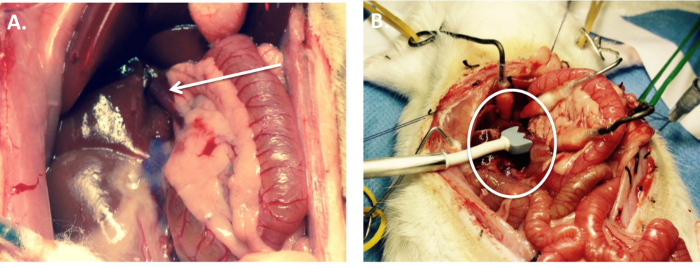
Figure 4: Intraoperative Measurement of Portal Vein Pressure and Volume Flow. (A) During the procedure, a needle pressure transducer is inserted into the exposed portal vein. (B) The 2 mm volume flow probe is used to measure volume flows in the main portal vein. Please click here to view a larger version of this figure.
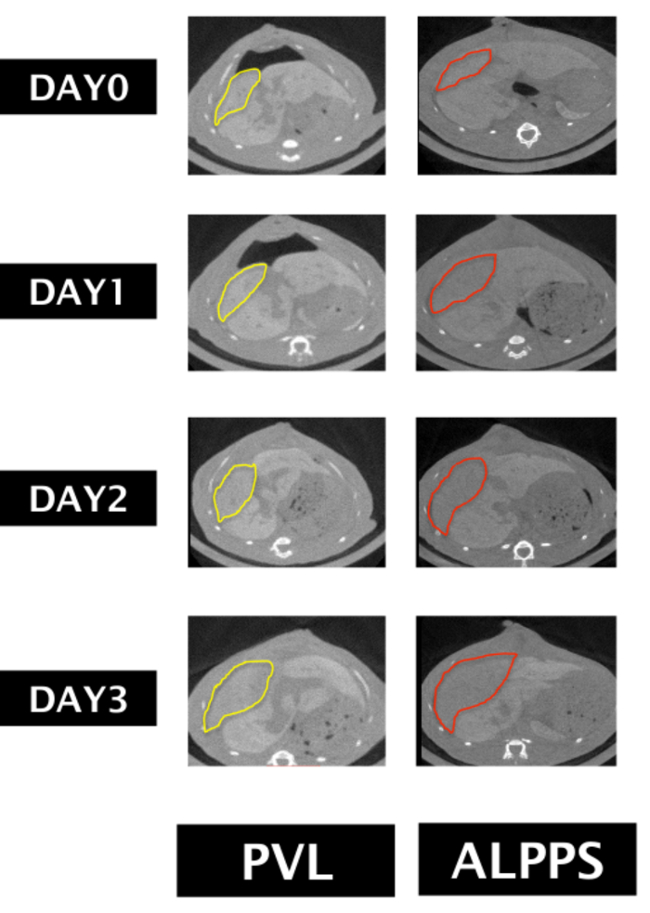
Figure 5: Liver Volumetry. The liver increases more in size after PVL+T than after PVL alone. The figure shows daily volumetry performed on digital imaging and communications in medicine (DICOM) files obtained with a rat micro CT scanner and using the public domain imaging platform. While the difference is obvious on axial images, quantitative volumetry as performed in a previous report17, shows a significant difference in growth kinetics. Please click here to view a larger version of this figure.
Discussion
This protocol presents an animal model of ALPPS with its rapid hypertrophy induced by PVL+T, that roughly doubles volume increase within 3 days compared to PVL alone.17 The right middle hepatic lobe is used as a model for the growing liver lobe because the middle hepatic lobe is one contiguous parenchymal mass supplied by two separate portal veins to its left and to its right side, as shown in Figure 1 in a recently published work.17 Compared to other reports, the model offers some advantages. Anatomically, the choice of the middle lobe best represents the human liver as one contiguous parenchymal mass that allows for transection and thereby obliteration of collateral flow. The branching of the portal vein to the left median lobe (LML) inside the left lateral lobe (LLL) allows for a combined ligation of LML and LLL.
There have been various rat and one murine model for ALPPS developed and described.18 Many rat models19,20 and the only mouse model15 described requires a liver mass reduction. Mass reduction may trigger enhanced hypertrophy independently. This is in contrast to our17 and similar rat models.14,21,22,23 The advantage of a murine model may be the use of genetically modified animals. Alternatively to these small animal models, a pig model has been developed,16 using a similar surgical technique as in humans and resulting in similar growth rates. Despite the fact, that this probably most closely resembles the human surgical procedure, small animal models may still be very important as they are faster, are easier to perform, allow larger number of animals per group and are less costly.
Physiologically, the rat model allows the study of blood flow, collateralization and oxygenation more easily than a mouse model. This study is the first to use the same methodology used clinically in humans to assess volume changes in the liver, namely CT volumetry. In contrast to some other studies, which do not include a control group (e.g. in a pig model of ALPPS24) yet assume ALPPS growth kinetics, we validated the hypertrophy by comparing PVL with PVL+T. While under PVL the RML doubles in within 3 days, PVL+T increases hypertrophy significantly. This acceleration of hypertrophy after 3 days by the added transection exactly mirrors the human condition, where a 46% volume increase has been reported in a large meta-analysis for PVE and an 86% increase in ALPPS after 10 days in the first large ALLPS registry report of 202 patients.25 Both the rat procedure PVL+T and human ALPPS double the amount of hypertrophy achieved in their respective time frames for the two procedure types.
Critical steps within this protocol include the dissection of the portal vein branches in PVL and the transection of the median lobe in PVL +T. During the dissection of the portal vein branches, it is important to disrupt the thin layer of peritoneum covering the entire hepatoduodenal ligament and not to push the instruments against resistance. An accidental tear in the portal vein may be stopped by pressure using cotton-swabs alone, but may be irreparable and require sacrifice of the animal. In general, it must be emphasized, that animals suffering from a blood loss of more than an estimated 10% of the animal's blood volume, should be excluded from the study, since this may alter the study results and cause unnecessary suffering of the animals.
Transection of the median lobe can be achieved by careful cauterization of the liver tissue using fine silver bipolar forceps and enough saline dripping, followed by simple cutting of the cauterized tissue using a scissors. The transection ought to be stopped prior to encountering the vena cava, which runs inside of the liver in rodents, to avoid massive bleeding and air embolism into the vena cava. Entry of air into the pulmonary circulation leads to sudden cardiac arrest in rats.
Troubleshooting of this protocol may include all modifications that lead to increase physiologic stress for the animals, such as hypotension induced by oversedation, hypothermia, increased blood loss and too long operative times. This protocol may well be modified for other rodent species like mice. We have successfully performed the technique described in this protocol in C57BL/6 mice (data not shown).
A limitation of this protocol is the exclusive use of this protocol to study the mechanisms of rapid versus slow hypertrophy; therefore the second stage of the "ALPPS" procedure, the resection of all deportalized liver tissue except for the hypertrophied liver, is not described in this protocol. This resection however can easily be achieved following standard technique of liver resection in rodents, using suture ligation and then removal of the liver lobes using a scissors.
Overall, this current model allows experiments elucidating the mechanism of rapid liver hypertrophy and testing of medications and interventions. Using this model, it was recently shown that rapid hypertrophy of the RML can also be induced by portal vein ligation in conjunction with hypoxia signaling using prolyl-hydroxylase inhibitors, suggesting that hypoxia signaling my play an important role in the modulation of liver growth kinetics. Drugs like prolyl-hydroxylase inhibitors may accelerate liver regeneration and should be further tested.17,26 Future applications of this model may be that the role of conventional and novel chemotherapeutic agents may be tested and their effect on the acceleration of liver regeneration may be further elucidated. The model also offers the opportunity to study liver function using for example indocyanine green (ICG) or hepatobiliary iminodiacetic acid (HIDA) scintigraphy in rats because ultimately slow and rapid volumetric changes will have to be put in the context of functional liver regeneration since liver function is more important than liver volume.27,28 The assessments of ALPPS patients with ICG29 and HIDA scintigraphy30,31 have so far only been tested in retrospective cohort studies, but these still may be very important tools for answering the question whether volume or function changes are similar or dissimilar in rapid liver regeneration.
In summary, we present a well characterized and standardized model of rapid and slow liver regeneration, that will allow future studies in regenerative liver surgery.
Declarações
The authors have nothing to disclose.
Acknowledgements
The authors have no acknowledgements.
Materials
| Isoflurane, 250ml bottles | Attane, Piramal, Mumbai, India | LDNI 22098 | Standard vet. equipment |
| Tec-3 Isofluorane Vaporizer | Ohmeda, GE-Healthcare, Chicago, IL | not available anymore | Standard vet. equipment |
| Buprenorphine (Temgesic) | Indivior, Baar, Switzerland | 7680419310353 | GTIN-number |
| Vitamine A ointment | Bausch&Lomp, Zug, Switzerland | 7680223980247 | GTIN-number |
| Atropine sulfate 0.5mg/ml | Sintetica SA, Mendrisio, Switzerland | 7680565330045 | GTIN-number |
| Microsurgery microscope | Olympus, Tokio, Japan | SZX10 | Standard vet. equipment |
| Betadine | Mundipharma, Basel, Switzerland | 7680342821377 | GTIN-number |
| Sponges | Carl Roth GmbH, Karlsruhe, Germany | NK83.1 | Mini-sponges |
| Abdominal Wall retractors | N/A | N/A | Self-made from paper clips and Q-Tips |
| 3-0 silk | Ethicon, Sommerville, NJ | K872H | Standard surgical |
| Scissors | World precision instruments (WPI), Sarasota, FL | 503371 | Standard microsurgical |
| Adson forceps | World precision instruments (WPI), Sarasota, FL | 501244-G | Standard microsurgical |
| Fine tips microforceps | World precision instruments (WPI), Sarasota, FL | 501976 | Tips need to be polished regularly |
| Curved fine tips microforceps | World precision instruments (WPI), Sarasota, FL | 504513 | Essential to go around the portal vein branches |
| 6-0 LOOK black braided silk | Surgical Specalities Corporation, Wyomissing, PA | SP114 | Spool, precut prior to the procedure |
| 2-0 silk sutures | Ethicon, Sommerville, NJ | K833 | Standard surgical |
| 5-0 maxon sutures | Covidien, Dublin, Ireland | 6608-21 | Standard surgical |
| Bipolar microforceps | Sutter, Freiburg, Germany | 780148SGS | Essential for parenchymal transection |
| Q-tips small | Carl Roth GmbH, Karlsruhe, Germany | EH11.1 | Standard surgical |
| Q-tips big | Carl Roth GmbH, Karlsruhe, Germany | XL54.1 | Standard surgical |
| G30 needle | Terumo, Tokyo, Japan | NN-3013R | Standard anesthesia equipment |
| 2mm volume flow probe | Transonic Systems, Ithaca, NY | MA-2PS | Smallest available probe for HAT-311 flow meter |
| Transonic flow meter | Transonic Systems, Ithaca, NY | HAT-311 Transsonic flow QC meter | One of the first generation flow flow meters for surgery |
| ExiTron nano 12,000 | Miltenyi Biotech, Bergisch Gladbach, Germany | 130-095-698 | Nanomoloecular contrast medium that opacifies liver and spleen |
| G26 intravenous catheter | Becton Dickinson, Franklin Lakes, NJ | 391349 | Standard anesthesia equipment |
| Quantum FX MicroCT | Perkin Elmer, Waltham, MA | N/A | Standard small animal CT scanner at the institute of physiology, University of Zürich |
| OsiriX 8.0 | Pixmeo Sarl, Geneva, Switzerland | N/A | Public domain software : www.pixmeo.com |
Referências
- She, W. H., Chok, K. Strategies to increase the resectability of hepatocellular carcinoma. World J Hepatol. 7 (18), 2147-2154 (2015).
- Vauthey, J. N., et al. Standardized measurement of the future liver remnant prior to extended liver resection: methodology and clinical associations. Surgery. 127 (5), 512-519 (2000).
- Kinoshita, H., et al. Preoperative portal vein embolization for hepatocellular carcinoma. World J Surg. 10 (5), 803-808 (1986).
- van Lienden, K. P., et al. Portal Vein Embolization Before Liver Resection: A Systematic Review. Cardiovasc Intervent Radiol. , (2012).
- Kianmanesh, R., et al. Right portal vein ligation: a new planned two-step all-surgical approach for complete resection of primary gastrointestinal tumors with multiple bilateral liver metastases. J Am Coll Surg. 197 (1), 164-170 (2003).
- Nadalin, S., et al. Volumetric and functional recovery of the liver after right hepatectomy for living donation. Liver Transpl. 10 (8), 1024-1029 (2004).
- Michalopoulos, G. K., DeFrances, M. C. Liver regeneration. Science. 276 (5309), 60-66 (1997).
- Fulop, A., et al. Alterations in hepatic lobar function in regenerating rat liver. J Surg Res. 197 (2), 307-317 (2015).
- Schnitzbauer, A. A., et al. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann Surg. 255 (3), 405-414 (2012).
- de Santibanes, E., Clavien, P. A. Playing Play-Doh to prevent postoperative liver failure: the "ALPPS" approach. Ann Surg. 255 (3), 415-417 (2012).
- Schadde, E., et al. Monosegment ALPPS hepatectomy: extending resectability by rapid hypertrophy. Surgery. 157 (4), 676-689 (2015).
- Dokmak, S., Belghiti, J. Which limits to the "ALPPS" approach?. Ann Surg. 256 (3), e6 (2012).
- Aloia, T. A., Vauthey, J. N. Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS): what is gained and what is lost?. Ann Surg. 256 (3), e9 (2012).
- Yao, L., et al. Establishment of a rat model of portal vein ligation combined with in situ splitting. PLoS One. 9 (8), e105511 (2014).
- Schlegel, A., et al. ALPPS: from human to mice highlighting accelerated and novel mechanisms of liver regeneration. Ann Surg. 260 (5), 839-846 (2014).
- Croome, K. P., et al. Characterization of a porcine model for associating liver partition and portal vein ligation for a staged hepatectomy. HPB (Oxford). 17 (12), 1130-1136 (2015).
- Schadde, E., et al. Hypoxia of the growing liver accelerates regeneration. Surgery. 161 (3), 666-679 (2017).
- Moris, D., et al. Mechanistic insights of rapid liver regeneration after associating liver partition and portal vein ligation for stage hepatectomy. World J Gastroenterol. 22 (33), 7613-7624 (2016).
- Garcia-Perez, R., et al. Associated Liver Partition and Portal Vein Ligation (ALPPS) vs Selective Portal Vein Ligation (PVL) for Staged Hepatectomy in a Rat Model. Similar Regenerative Response?. PLoS One. 10 (12), e0144096 (2015).
- Shi, H., et al. A preliminary study of ALPPS procedure in a rat model. Sci Rep. 5, 17567 (2015).
- Almau Trenard, H. M., et al. Development of an experimental model of portal vein ligation associated with parenchymal transection (ALPPS) in rats. Cir Esp. 92 (10), 676-681 (2014).
- Dhar, D. K., Mohammad, G. H., Vyas, S., Broering, D. C., Malago, M. A novel rat model of liver regeneration: possible role of cytokine induced neutrophil chemoattractant-1 in augmented liver regeneration. Ann Surg Innov Res. 9, 11 (2015).
- Wei, W., et al. Establishment of a rat model: Associating liver partition with portal vein ligation for staged hepatectomy. Surgery. 159 (5), 1299-1307 (2016).
- Tschuor, C., et al. Salvage parenchymal liver transection for patients with insufficient volume increase after portal vein occlusion – an extension of the ALPPS approach. Eur J Surg Oncol. 39 (11), 1230-1235 (2013).
- Schadde, E., et al. Early survival and safety of ALPPS: first report of the International ALPPS Registry. Ann Surg. 260 (5), 829-836 (2014).
- Harnoss, J. M., et al. Prolyl Hydroxylase Inhibition Enhances Liver Regeneration Without Induction of Tumor Growth. Ann Surg. , (2016).
- Olthof, P. B., et al. Comparable liver function and volume increase after portal vein embolization in rabbits and humans. Surgery. 161 (3), 658-665 (2017).
- Olthof, P. B., van Gulik, T. M., Bennink, R. J. Optimal use of hepatobiliary scintigraphy before liver resection. HPB (Oxford). 18 (10), 870 (2016).
- Lau, L., Christophi, C., Muralidharan, V. Intraoperative functional liver remnant assessment with indocyanine green clearance: another toehold for climbing the "ALPPS". Ann Surg. 261 (2), e43-e45 (2015).
- Cieslak, K. P., et al. Assessment of Liver Function Using (99m)Tc-Mebrofenin Hepatobiliary Scintigraphy in ALPPS (Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy). Case Rep Gastroenterol. 9 (3), 353-360 (2015).
- Truant, S., et al. Drop of Total Liver Function in the Interstages of the New Associating Liver Partition and Portal Vein Ligation for Staged Hepatectomy Technique: Analysis of the "Auxiliary Liver" by HIDA Scintigraphy. Ann Surg. 263 (3), e33-e34 (2016).
