The described implementation of a set-up for reliable repeated tES in alert rodents can be easily integrated into mechanistic experiments, dose-response studies, or experiments including behavioral tasks. To date, the comparability of data from animal studies using (noninvasive) tES is hindered by the variability of the tES stimulation set-ups between laboratories and by differences in stimulation parameters (e.g., various current densities applied at exorbitant high levels compared to the human application). Hence, the informative value of animal research in the field of tES is limited. This article presents a tES set-up which is easy to standardize across laboratories by implementing the placement of the "active" electrode on the bone above the targeted cortex (here, above the primary motor cortex (M1)) with saline as the preferable conductive medium and the counter electrode placed on the chest (externally or implanted).
Given the small size of rodents, placing the electrode above the targeted cortex on the rodent's skin may lead to excessive shunting, particularly when the counter-electrode is placed in close proximity, e.g., in the neck (for examples of current modeling, see Figure 3 (adopted from reference1)). Additionally, the stability and electrode contact is less reliable and rodents are more irritated by repeated electrode placement on the scalp when using a transdermal application. The fixation of a non-permanent set-up may also hinder the rodent from performing freely. In contrast, the rodents adjust quickly to this permanently present implanted set-up.
The estimation of an equivalent stimulation intensity compared to human stimulation parameters is difficult, since models can only take into account a limited numbers of factors and rodents are pachygyric (see reference1 for estimation of a scaling factor). Therefore, collecting dose-response data including low intensity currents may be most informative. Using the presented surgical set-up in a dose-response study in anesthetized rats, the dose-dependent microglial activation outlasting the stimulation period (24 h post-stimulation) was demonstrated and dissociable from neurodegeneration occurring at high intensity DCS (Figure 4; adopted from reference17). Microglial activation, assessed by morphological alteration, occurred first at 31.8 A/m² (Figure 4C), while the first signs of neurodegeneration were detected at 47.8 A/m². In these experiments, the anesthesia clearly affected the magnitude of response to DCS as the percentage of brain slices with fluorojade C (FJC) positive degenerating neurons in alert rats was higher at 47.8 A/m² (Figure 4A). As the threshold for ≥ 24 h lasting microglial activation is close to the lesion threshold, but greatly above the intensities that promote physiological cognitive and plastic processes in humans, such activation might rather indicate a pre-lesional inflammation induced by DCS. Hence, behavioral or molecular effects of DCS at these high intensities are expected to be mechanistically different compared to low intensity effects (see the scheme summarizing effects and intensities of tDCS experiments in Figure 5).
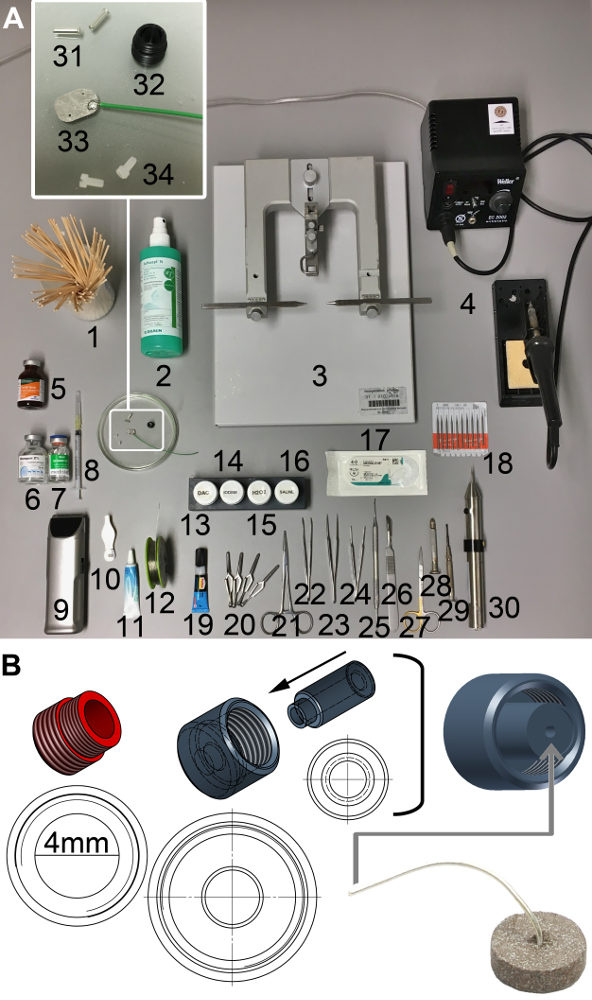
Figure 1: Supplies for surgery and technical scheme of the tES socket and electrode cap unit. (A) 1. Cotton swabs, 2. disinfectant, 3. stereotactic frame, 4. soldering iron, 5. analgesic (e.g., carprofen), 6. & 7. anesthetics (e.g., xylazine & ketamine), 8. syringe, 9. clipper, 10. ear puncher, 11. eye ointment (e.g., bepanthene), 12. lead-free tin-solder, 13. two-component dental acrylic cement (DAC), 14. iodine, 15. 3% H2O2, 16. 0.9% saline, 17. synthetic braided non-absorbable suture (e.g., Mersilene 4-0), 18. drill bits, 19. cyanoacrylic glue, 20. bulldog clamps 21. homeostatic forceps, 22. bent, serrated tip forceps, 23. straight, sharp tip forceps, 24. straight, tissue forceps, 25. dental spatula, 26. scalpel, 27. scissors, 28. hand drill, 29. screw driver, 30. motor driven drill, 31. female connectors, 32. tES socket, 33. square platinum electrode attached to cable, soldering joint covered with histoacrylic glue, 34. plastic screws. (B) tES socket (red) for fixation on the rodent skull with an inner diameter of 4 mm; the electrode unit (grey) is built by a screw cap and an inner stamp with a center hole leaving room for the cable of the Ag/Cl disc electrode, which is glued to the bottom of the stamp. This allows for maximal stability of the set-up and avoidance of wire breaks at the sensitive wire-electrode-connection point. Please click here to view a larger version of this figure.
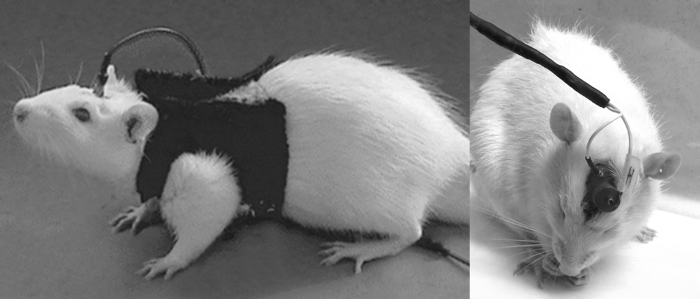
Figure 2: Rats equipped with tES set-up. The rat on the left is equipped with an externally fixed counter electrode on the shaved chest. The carbon rubber electrode is sewed to the bottom of the vest. The rat on the right has an implanted chest electrode with the cable tunneled to the head. The female connector attached to the cable (caudal) is fixed within the dental acrylic cement built unit, behind the socket for the tES electrode (rostral). Please click here to view a larger version of this figure.
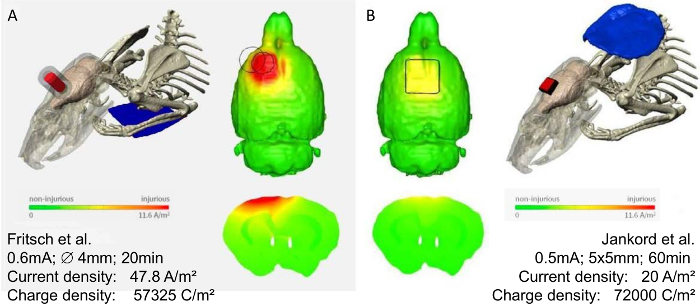
Figure 3: Modeling of current distribution in two different rodent tES montages. Finite element models predicting the brain current flow in two rat models with epicranial tDCS montages, modified with permission1. Using these models, the predicted threshold brain current density to induce cortical lesions was 17.0 A/m² for the montage used by Fritsch, et al.8 (A), and 6.3 A/m² for the montage by Rohan, et al.21 (B), corresponding to electric fields of 61, and 23 V/m, respectively. Note the discrepancies in the current flow pattern of the two different montages. In (A) a higher current density for a shorter time is applied, resulting in a lower charge density than in (B). Most importantly the placement of the counter electrode (neck vs. chest) might have an additional impact on the resulting brain current flow. Therefore, for interpretation of rodent data, the specification of electrode size, placement (both electrodes), applied current, and stimulation duration is necessary. Note that the actual current within the rat brain can only be estimated by using these computational models. Color scale indicates current density from zero to 11.6 A/m², and above. Please click here to view a larger version of this figure.
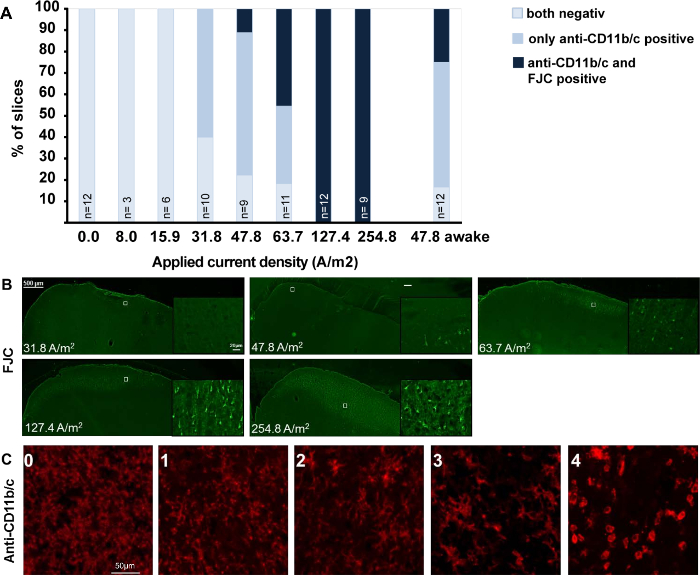
Figure 4: Dose response effects of DCS on microglia activation and neurodegeneration in brain slices obtained after different doses of anodal tDCS applied to the primary motor cortex. The figure is modified from17 summarizing the immunohistological findings of a dose-response tDCS study. (A) Relation between morphologically activated microglia assessed by anti-CD11b/c staining (rating see below) and neurodegeneration revealed by FJC positivity. Rat motor cortical brain slices were rated by a blinded investigator either as anti-CD11b/c and FJC staining negative, as anti-CD11b/c positive only (detection of activation determined morphologically), or as both anti-CD11b/c and FJC positive. Note that microglial activation preceded occurrence of neurodegeneration. (B) Representative coronal sections of left motor cortical brain slices (at or near +1.56 mm from the bregma) from rats exposed to different intensities of anodal tDCS applied to the primary motor cortex. In anesthetized rats, no signs of neurodegeneration occurred at 31.8 A/m², while a few degenerating neurons were present at 47.8 A/m² and neuronal damage further increased with increasing dose. Of note, anodal DCS at 47.8 A/m² in alert rats increased the percentage of slices with neurodegeneration. Scale bar for all sections: 500 µm. Magnification inlet scale bar for all sections: 20 µm. (C) Histological sample images of the rating of microglia activation in anti-CD11b/c immunohistochemistry, ranging from 0 (not activated) to 4 (severely activated), 1-4 were rated as "positive". Scale bars = 50 µm. Please click here to view a larger version of this figure.
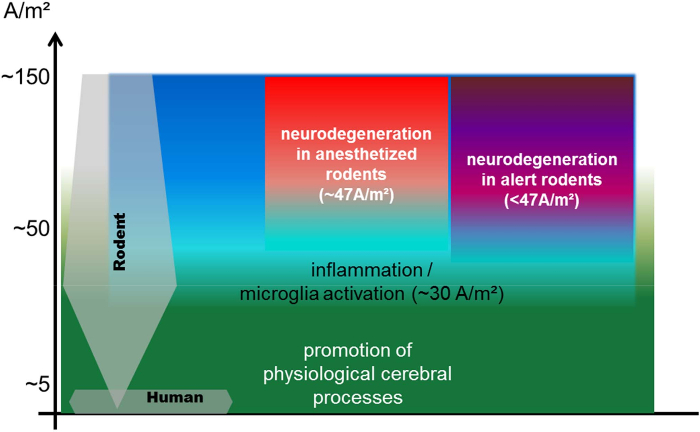
Figure 5: Scheme illustrating the relation of currently used rodent tDCS current densities compared to the human application: thresholds for inflammation, neurodegeneration, and modulation of physiological processes at stimulation durations of up to 30 min. The currently used rodent DCS current densities range from 1.3 to 143 A/m² with the majority of studies using more than 20 A/m², while the current densities in the majority of human studies are between 0.3 and 0.8 A/m²1,14. Human stimulation parameters are at least one order of magnitude below the threshold for neurodegeneration1. Threshold for neurodegeneration is significantly higher under anesthesia, when cortical excitability is suppressed17. Lasting microglial activation begins below but close to the intensities inducing neuronal damage17. Investigation of modulating effects of DCS on physiological cerebral processes at higher intensities below the lesion threshold are likely different from theses seen at very low intensities (comparable to the human application). The exact translation of stimulation parameters between species is under investigation. Estimations are hindered by passive factors like size and anatomy (sulci and gyri), but also by possible different sensitivities to electric fields of neurons, glia, and networks across species (it is not known whether the same current flow would lead to the same physiological effect). Therefore, the most informative study design is testing tES effects in a dose response manner, including very low current intensities. The scheme is based on data from7,12,16,18,19,20,21,22,23,24,25,26,27,28,29,30,31 (maximum stimulation duration of 30 min per session, data are from disease animal models excluded). Please click here to view a larger version of this figure.
