First, the success of the surgical procedure can be confirmed by analysis of the MRI scans (see example in Figure 2). All four pins should be located in the middle of the femoral shaft. The size of the osteotomy gap should be between 0.3-0.5 mm. If the size of the osteotomy gap varies greatly from these values, the mouse should be excluded from further analysis.
Secondly, the evaluation of longitudinal scans during the fracture healing process in the same animal provides information about callus tissue development. If mice are scanned at day 10, 14, and 21 (see example in Figure 3), cartilaginous tissue is visible in the middle of the fracture callus on day 10 (relative cartilage area = 30.8%) and day 14 (relative cartilage area = 29.0%), and decreases until day 21 after surgery (relative cartilage area = 10.5%) (Figure 3). Bony tissue is visible at the periphery of the fracture callus on day 10 (relative bone area = 7.2 %), increases until day 14 (relative bone area = 15.6%), and body bridging occurs until day 21 (relative bone area = 45.7%).
Thirdly, after segmentation of the different tissues in the fracture callus using image analysis software, 3D images from the fractured femur and the fracture callus can be generated. In the example shown in Figure 4, a whole femur scanned on day 26 after fracture is displayed. Mature cortex is marked in grey, the ceramic pins are marked in yellow, callus soft tissue is marked in green, cartilage tissue is marked in red, and callus bony tissue is marked in purple.
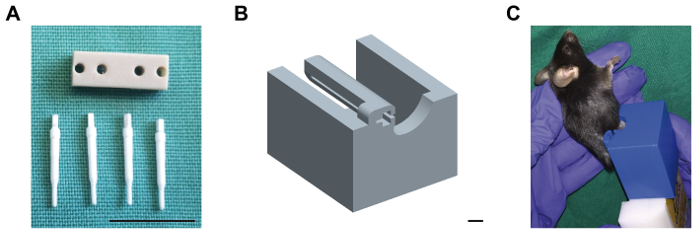
Figure 1: External fixator with ceramic mounting pins and MRI mounting device. (A) The plastic body of the external fixator is shown, as well as the four ceramic mounting pins which are compatible to MRI scans. Scale bar: 1 cm. (B) The computer-aided drawing of the custom-made mounting device for insertion of the external fixator during MRI scans is shown. The external fixator at the right femur of the mouse is inserted into the relief of the mounting device. Then, the device is plugged on the four-element head coil prior to scanning. Scale bar: 0.4 cm. (C) Mouse placed in the mounting device (blue), attached to the 4-element head coil (white). Please click here to view a larger version of this figure.
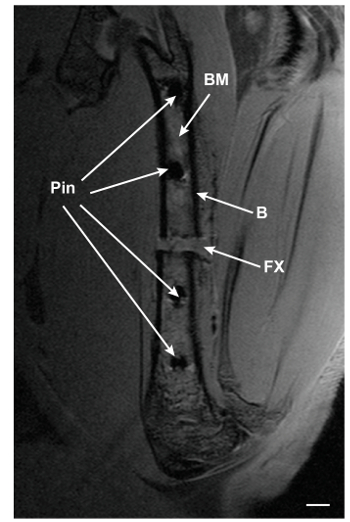
Figure 2: PD-TSE MRI image of a fractured femur 3 days after surgery. A central slice of a fractured femur scanned on day 3 after surgery is shown. BM: bone marrow; B: bone; FX: fracture gap. Scale bar: 0.5 mm. Please click here to view a larger version of this figure.
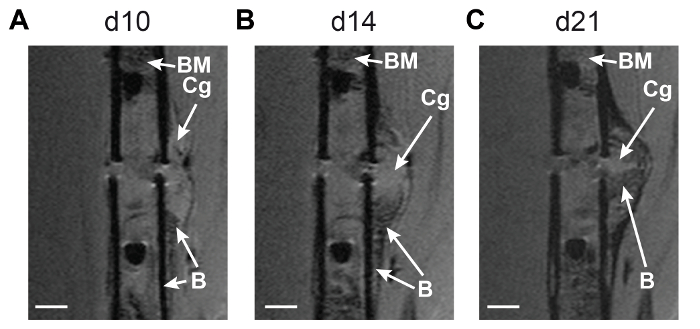
Figure 3: Longitudinal monitoring of fracture callus development using MRI technique. Central MRI slices from the fractured femur of one mouse scanned on (A) day 10, (B) day 14, and (C) day 21 after surgery are displayed. Hyper-intense cartilaginous tissue is visible in the middle of the fracture callus on day 10 and day 14, and decreases until day 21 after surgery. Hypo-intense bony tissue is visible at the periphery of the fracture callus on day 10, increases until day 14, and body bridging occurs until day 21. BM: bone marrow; Cg: cartilaginous tissue; B: bony tissue. Scale bar: 0.5 mm. Please click here to view a larger version of this figure.
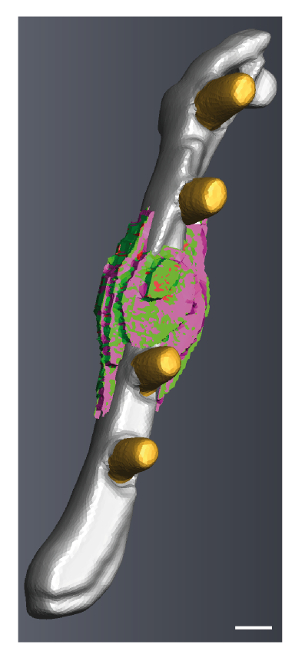
Figure 4: 3D reconstruction from a fractured femur scanned on day 26 after surgery. Mature cortex is marked in grey, the ceramic pins are marked in yellow, callus soft tissue is marked in green, cartilage tissue is marked in red, and callus bony tissue is marked in purple. The image was generated using image analysis software. Scale bar: 0.4 mm. Please click here to view a larger version of this figure.
