The vrRSB was tested in 156 twin pairs epidemiologically ascertained from the Missouri Family Register as part of the Early Reciprocal Social Behavior Study, a prospective, longitudinal study of the development of RSB12. We selected a twin study design to examine whether the vrRSB could detect individual differences in RSB within toddlers from the general population and whether this variation was heritable. Both these features have been demonstrated with the SRS in older children5,8 and are key for evaluating the vrRSB's ability to capture genetically informative variance in RSB which is relevant for both typical and atypical development.
Caregivers completed behavioral measures on the twins at 18, 24, 36, and 48 months of age; the vrRSB (primarily the hard-copy version, as the online version was developed later in the study) was collected at the 18- and 24-month time points. The sample was primarily Caucasian (80.1%) and non-Hispanic (91.6%), similar to the Missouri population23, whereas median annual household income of the sample ($60,001 – $90,000) was higher than that of Missouri ($47,200). Informal feedback from participants regarding the survey was generally positive, with over 95% of returned surveys being correctly completed. To account for non-independence of twin data, analyses of reliability, behavioral correlations, and longitudinal differences included data from one twin selected at random. One child, who underwent a developmental regression and ultimately received a community diagnosis of ASD, was excluded from these twin analyses.
Both the Video-referenced Scores and the RSB Total Score demonstrated a continuous, unimodal distribution at 18 and 24 months across the general population sample (Figure 1). For the Video-referenced Score, a greater preponderance of lower scores at 24 months of age suggested a slight floor effect due to more advanced development (higher scores indicate less RSB). Distributions of the RSB Total Score, like those for the SRS3, were right-skewed, reflecting the small proportion of individuals with significant deficits in RSB. Similar score distributions have been observed in an independent sample of primarily Hispanic, bilingual twins from California (unpublished data, Harris, B., 2017).
Good internal reliability for both video-referenced items and the RSB Total score was observed at 18 months (Cronbach's alpha Video-referenced Score = .841, p <.001; Cronbach's alpha RSB Total Score = .879, p <.001) and 24 months (Cronbach's alpha Video-referenced Score = .881, p <.001; Cronbach's alpha RSB Total Score = .868, p <.001). The strong internal consistency suggests that these item indices represent cohesive constructs throughout toddlerhood.
Test-retest reliability was calculated according to intraclass correlation coefficients (ICCs; two-way mixed single measures) based on scores obtained at the 18- and 24-month time points. Good 6-month test-retest reliability was observed for the Video-referenced Score (ICC(3,1) = .505, p <.001, Figure 2a), and strong test-retest reliability was observed for RSB Total Score (ICC(3,1) = .735, p <.001; Figure 2b).
In addition to demonstrating test-retest reliability and, by extension, the capacity to detect trait-related consistency in RSB across time, an important goal for the vrRSB was to track progress in RSB over development. Both the Video-referenced and RSB Total Score were able to detect significant improvement in RSB over time, manifested by decreased scores (lower scores signify better RSB) between 18 and 24 months (Table 2). Video-referenced Scores showed a larger effect size for these decreases vs. the RSB Total Score (Cohen's d = 0.66 vs. 0.48). Separate calculations for the non-video-referenced items (Table 2), which were not designed to track change, revealed a much smaller effect size for these items (Cohen's d = 0.22).
Since variation in RSB has been shown to be heritable in older populations, twin-twin concordances were calculated for Video-referenced Scores and RSB Total Scores at 18 months (Table 3). Higher intraclass correlations in monozygotic (identical) twins, who share all their genetic material, vs. dizygotic (fraternal) twins, who share on average half of their genetic material, are consistent with heritability of RSB. Concordances for monozygotic twins were quite high and in many cases roughly double those of dizygotic twins, supporting a strong role for genetic influences. Of note, monozygotic twin concordances also indicate of the upper limit of possible measurement error. For both vrRSB scores, the possible measurement error is less than 9% at the level of the entire twin sample (error = 1 – monozygotic twin concordance).
As a test of concurrent validity, we examined correlations of scores on the M-CHAT, a screener for ASD, with the vrRSB. Positive correlations were consistent with the vrRSB's capacity to capture variation related to ASD risk (Video-referenced Score: r = .444, p <.001; RSB Total Score: r = .654, p <.001). We also obtained correlations between vrRSB scores and expressive vocabulary (percentile scores) as measured by the MacArthur-Bates Communicative Development Inventory Short Form24, given an anticipated relationship between language and social communication. Significant correlations were found for both the Video-referenced Score (r = -.419, p <.001) and the RSB Total Score (r = -.309, p <.001).
Lastly, in pilot testing (Table 4), we compared scores for twins without a diagnosis of ASD and a small sample of children with either a community diagnosis of ASD or a rating of autism or autism spectrum on the Autism Diagnostic Observation Schedule21 (mean age(SD): 24.75(5.56) months; age range: 17 – 33 months). Both Video-referenced Scores and RSB Total Scores differentiated between children with and without ASD, with an effect size (Cohen's d) of -1.39 for the video-referenced score and -1.66 for the RSB Total Score. Group differences were also observed on item scores for ASD core symptom domains (Social Communication: Cohen's d = -1.58; Restricted, Repetitive Behavior: Cohen's d = -1.52). At the level of quantitative RSB scores, both the 18-month Video-referenced Score and RSB Total Score were correlated with total scores on the 36-month SRS (Video-referenced Score: r = .298, p = .001; RSB Total Score: r = .624, p <.001).
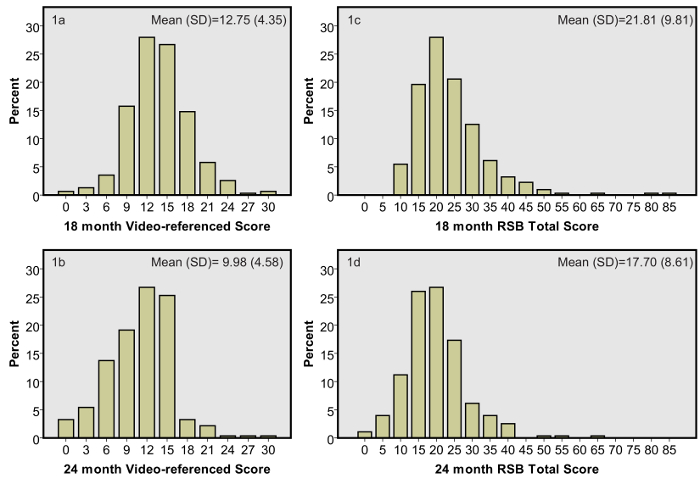
Figure 1: Continuous Unimodal Score Distributions for Video-referenced Score and RSB Total Score at 18 and 24 months
Panels illustrate scores for the vrRSB, including both Video-referenced Score and RSB Total Score, which is comprised of video-referenced items plus traditionally presented survey items adapted from the Social Responsiveness Scale. These distributions are based on a sample of twins ascertained from the general population (n = 156 pairs). Panels 1a and 1b show scores for video-referenced items at 18 and 24 months while panels 1c & 1d show RSB Total Scores at 18 and 24 months. In all cases, scores are continuously distributed and unimodal, consistent with RSB operating as a dimensional construct in toddlers. Means and standard deviations (SD) are indicated for each time point in upper right of panel. Please click here to view a larger version of this figure.
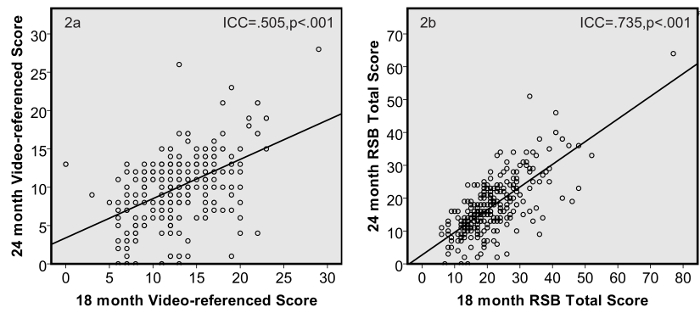
Figure 2: 6-month Test-Retest Reliability for Video-referenced Score and RSB Total Score
Scatterplots illustrate a cross-time comparison at 18 and 24 months for subjects' Video-referenced Score (2a) and RSB Total Score (2b). Intraclass correlation coefficients (ICC(3,1)) show good test-retest reliability for the Video-referenced Score and strong test-retest reliability for RSB Total Score. Please click here to view a larger version of this figure.
| Classification of Forward- and Reverse-Scored Items | |||||||||||
| Forward-Scored Items | 15 – 16, 18 – 26, 28 – 34, 36, 40 – 41, 47, appendix item 1 | ||||||||||
| Reverse-Scored Items | 1 – 13; 14, 17, 27, 35, 37 – 39, 42 | ||||||||||
| Point Values for Item Ratings | |||||||||||
| Video-referenced Items | Non-video Referenced Items | ||||||||||
| Rating option | Not at all | Somewhat but less than child in video | About the same as child in video | More than child in video | Not true | Sometimes true | Often true | Almost always true | |||
| Forward- scored | None | 0 | 1 | 2 | 3 | ||||||
| Reverse-scored | 3 | 2 | 1 | 0 | 3 | 2 | 1 | 0 | |||
| Item Lists for Main Scores and Subscale Scores | |||||||||||
| Scale/Subscale | Item numbers | Score ≥2 SD of Mean | |||||||||
| 18 months | 24 months | ||||||||||
| RSB Total | 1 – 13;14 – 42; 47; appendix item 1 | 41 | 35 | ||||||||
| Video-referenced | 1 – 13 | 21 | 19 | ||||||||
| Social Communication | 1 – 15; 17; 19; 21; 25 – 28; 30; 32 – 33, 35 – 40, 42, appendix item 1 | 36 | 32 | ||||||||
| Restricted Repetitive Behavior | 16, 18, 20, 22 – 24, 29, 31, 34, 41, 47 | 7 | 5 | ||||||||
Table 1: Guidelines for Video-referenced Rating of Reciprocal Social Behavior (vrRSB) Scoring
This table provides a breakdown of item types, point values, and item lists used for scoring. The vrRSB contains 2 main scores, the RSB Total Score and the Video-Referenced Score, and 2 subscale scores, Social Communication and Restricted Repetitive Behavior, which include items related to the 2 core symptom domains of ASD. These scores quantify the level of deficits in RSB and thus also indicate the burden of core autistic symptoms. Note that select items address aspects of general development, and these items are not included in scoring. Items 49 and 50 provide an indication of the achievement of two key language milestones for toddlers: the use of spoken language and combining words into phrases or sentences. Item 43 regards unusual sleep patterns, with greater endorsement suggesting a less typical developmental profile. For items regarding spatial abilities (44, 48) and intellectual curiosity (45, 46), greater endorsement corresponds to more advanced development.
| Paired Samples | Paired Differences | T | df | Sig. | ||||
| Mean | Standard Deviation | Standard Error Mean | 95% Confidence | |||||
| Interval | ||||||||
| Lower | Upper | |||||||
| 18m Video-referenced Score – | 2.91 | 4.38 | 0.37 | 2.17 | 3.64 | 7.79 | 137 | <.001 |
| 24m Video-referenced Score | ||||||||
| 18m RSB Total Score – | 4.30 | 6.48 | 0.55 | 3.21 | 5.40 | 7.80 | 137 | <.001 |
| 24m RSB Total Score | ||||||||
| 18m non-video items – | 1.40 | 4.47 | 0.38 | 0.65 | 2.15 | 3.68 | 137 | <.001 |
| 24m non-video-items | ||||||||
Table 2: Differences in Video-referenced Rating of Reciprocal Social Behavior (vrRSB) scores from 18 to 24 months
Paired t-tests are used to calculate differences between scores at 18 and 24 months (n = 138). Score differences are for Video-referenced Scores, RSB Total Scores, and scores for the non-video referenced items (RSB Total Score – Video-referenced Score). vrRSB indicates Video-referenced Rating of Reciprocal Social Behavior. Df indicates degrees of freedom. Sig. indicates significance.
| Twin Type (pairs) | Video-referenced | RSB Total |
| MZ (n = 54) | .928 (p <.001) | .912 (p <.001) |
| DZ (n = 95) | .388 (p <.001) | .218 (p <.001) |
| Male MZ (n = 28) | .894 (p <.001) | .914 (p <.001) |
| Male DZ (n = 30) | .348 (p = .028) | .286 (p <.059) |
| Female MZ (n = 26) | .956 (p <.001) | .878 (p <.001) |
| Female DZ (n = 29) | .660 (p <.001) | .369 (p <.023) |
| Opposite Sex (n = 36) | .301 (p = .035) | .062 (p = .358) |
Table 3: Twin-Twin Concordances for Toddler Reciprocal Social Behavior at 18 months
Twin-twin concordances [ICC(3,1)] for Video-referenced Scores and RSB Total Scores at 18 months are shown for monozygotic (MZ) and dizygotic (DZ) twins. Values are reported for all MZ and DZ twin pairs grouped together as well as twin pairs analyzed separately by gender. Seven unclassified pairs were not able to be included in these analyses.
| no-ASD (n=310) | ASD (n=14) | Mean Difference | T | Df | Sig. | |
| Mean (SD) | Mean (SD) | |||||
| Video-referenced | 12.77 (4.44) | 21.86 (8.09) | -9.08 | -4.17 | 13.36 | 0.001 |
| RSB Total | 21.84 (9.79) | 56.79 (28.17) | -34.95 | -4.63 | 13.14 | <.001 |
| Social Communication | 20.15 (8.14) | 44.57 (20.16) | -24.42 | -4.52 | 13.19 | 0.001 |
| Restricted, Repetitive Behavior | 1.68 (2.76) | 12.21 (9.37) | -10.53 | -4.20 | 13.10 | 0.001 |
Table 4: Comparison of Video-referenced Rating of Reciprocal Social Behavior (vrRSB) Scores for Toddlers with and without autism spectrum disorder (ASD)
Means, mean differences and results of t-tests for vrRSB scores are shown for comparison of scores between twins without an ASD diagnosis and a small group of children with ASD. SD indicates standard deviation. Df indicates degrees of freedom. Sig. indicates p-values for 2-tailed significant differences.
Appendix 1: Copy of the Video-Referenced Rating Scale of Reciprocal Social Behavior Please click here to download this file.
