This protocol describes a test system developed for the detection of RNA fusion variants for use in the measurement of driver mutations within the plasma of NSCLC patients (Figure 1A). Fusion mRNA products from the expression of the most common RET and ROS1 rearrangements in the NSCLC population were identified13,14,15,16,17. Multiplexed PCR assays were then designed to detect the eight most common transcript variants for each target in NSCLC within a single reaction. The most common translocations at the ROS1 locus generate associations with the 5' portions of the CD74, SDC4, SLC34A2, EZR or TPM3 genes (Figure 1B). The most common translocations at the RET locus lead to juxtaposition with KIF5B, for which the assay covers six exon junctions. Additional RET partners that are covered include those with CCDC6 and TRIM33 (Figure 1C). In total, the assays cover approximately 88% of ROS1 and 99% of RET alterations known to occur in the NSCLC patient population17.
The specificity of the assay components was first evaluated using eight individual in vitro RNAs that contain the mRNA sequence for the fusion transcripts covered by the ROS1 or RET multiplexed assays. Each RNA species was tested against each individual variant assay that comprises the multiplexed version. There was no cross-reactivity of these assays, thus demonstrating 100% analytic specificity within the designed multiplexed assays (data not shown). To determine the lower limit of detection of the test protocol, total RNA derived from cell lines expressing a fusion variant included in the assay were mixed into a background of normal RNA at 5%, 1%, 0.2%, and 0.04% concentrations. The multiplexed RET and ROS1 variant PCR assays detected as little as 0.2% fusion variant (Figure 2A-B). Additionally, a preparation of 5% off-target cell line derived RNA (expressing an EML4-ALK fusion transcript) was not detected with the multiplexed ROS1 and RET assays, further demonstrating specificity (Figure 2A-B).
Precision testing of the RT-dPCR process was performed for both ROS1 and RET. Analytic control material comprised of equimolar in vitro RNAs was processed at three concentrations (High, Medium, and Low) through reverse transcription and dPCR on three different occasions within the same day (intra-day), on three consecutive days (inter-day), and with two operators (inter-operator). Results from precision testing demonstrated accurate detection of both the fusion transcript of interest, as well as a control gene, GUSB, which is included as an internal QC metric (Figure 2C–D).
In addition to the GUSB internal control, each batch of clinical samples was run with a set of batch controls. A positive control was developed from a mixture of analytic in vitro RNA that represented each of the fusion variants tested in RT-dPCR, as well as analytic in vitro RNA for GUSB. This RNA was spiked into normal human plasma lysate during RNA extraction and was processed alongside the clinical samples throughout the protocol. The no reverse transcriptase (No RT) control was a negative control to confirm the absence of contaminating material in the RNA extraction workflow and demonstrate the specificity of the primers for RNA. The No RT control was generated using the same material as the positive control, but it does not include enzyme within the cDNA synthesis reaction. The no RNA control (NRC) is a negative control to confirm the absence of contaminating transcripts in the reverse transcription reaction components. This control was introduced into the workflow at the cDNA synthesis step, and water was added in the reaction instead of an RNA template. The No RT and NRC controls must be negative in both channels, if accurate results are to be delivered. Table 1 lists the reverse transcription reaction components for each control. Examples of the 2D plots for each of these controls are shown for the ROS1 (Figure 3 A-C) and RET (Figure 3 E-G) multiplex assays. Fusion variants were detected using a fluorescein amidite (FAM) probe and are represented along the y-axis, while the control gene, GUSB, was detected using a 5'-hexachloro-fluorescein-CE phosphoramidite (HEX) probe and is on the x-axis. These batch controls were assessed over the course of 21 days to determine assay robustness. Fusion positive droplets and GUSB control gene droplets were observed for ROS1 and RET in all 21 runs executed over the course of the study (Figure 3D,H). All negative controls (No RT and NRC) yielded negative results across the entire 21 days (data not shown).
The ability to troubleshoot is a critical component of any test protocol to be run in the clinical laboratory setting. Here, we provide real world examples of sub-optimal results using the RT-dPCR protocol. The first is an example 2D plot demonstrating the importance of the no reverse transcriptase control (Figure 4A). In this example, mutant positive droplets were present even though there was no cDNA conversion due to lack of enzyme. This outcome was likely due to dPCR primers amplifying off-target genomic DNA. In this case, design of an intron-spanning assay will prevent amplification of genomic DNA. Alternatively, an RNase-free DNase enzyme can be used to eliminate the contaminating DNA, but this is not recommended for detection of rare targets, as some RNA degradation may occur during incubation with the enzyme. The next example 2D plot was a NRC with positive droplets in both channels (Figure 4B). This indicated contamination at some point in the RT-dPCR setup. In this case, the recommendation is to discard any potentially contaminated reagents used in testing, thoroughly decontaminate all equipment, and re-test with fresh reaction components. The third example 2D plot presented as a spray of droplets along a 45° line (Figure 4C). This is often caused by shearing and coalescing of droplets. Careful droplet handling prior to thermal cycling is essential, as droplets are prone to damage. We recommend the use of automated droplet generation, when available. If transferring manually generated droplets, be certain to choose the recommended wide-bore tips and employ careful pipetting technique. Droplet transfer requires slow aspiration and dispensing, with each taking place over 5-6 seconds, and it is essential that the pipette tip opening does not touch the droplet cartridge or well. When dispensing, keep the pipette tip at the liquid level and raise it slowly as droplets are dispensed (view video for demonstration). The final 2D plot example demonstrates a lack of separation between the positive and negative droplet populations (Figure 4D). This can have several causes. Strong PCR inhibitors, such as detergents used in lysis buffers and an excess of highly degraded DNA, can cause loss of separation. In this case, consider adding a clean-up step between cDNA synthesis and dPCR (such as described within Step 5 of this protocol). Finally, lack of separation can also be due to sub-optimal amplification conditions, and optimization of the PCR step should also be considered.
Data within Figure 5 represent 984 real world patient sample turn-around times and demonstrates the rapid nature of this test workflow. Results were reported to the treating physician as early as within 48 hours (79% of cases) of sample receipt and in 95% of cases, within 72 hours. In conclusion, the use of stabilized circulating RNA blood collection tubes, optimized RNA extraction procedures from blood, and RT-dPCR run according to an optimized protocol with the appropriate internal and batch controls, can provide a rapid test system for the accurate detection of fusion RNA variants relevant in NSCLC.
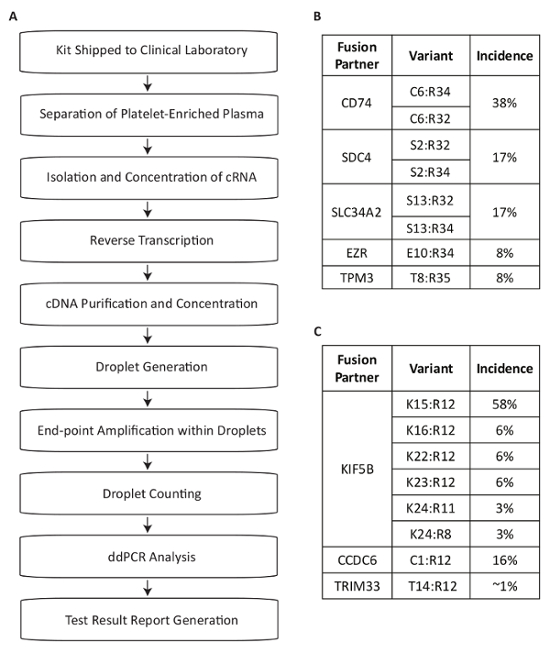
Figure 1: Overview of Blood Sample Processing Steps for Fusion Variant Detection using Assays Specific to the Most Prevalent RET and ROS1 Variants in NSCLC. (A) Sample testing is initiated when whole blood is drawn and a BCT is shipped within the specimen collection kit to the Clinical Laboratory. Circulating RNA is recovered from multiple sources within the platelet-enriched plasma, reverse transcribed with gene specific priming, and purified for use in dPCR. Samples are processed using a commercially available system which consists of droplet generation (emulsion), amplification, and droplet counting. Data is analyzed using commercially available software. The test results are then documented and reported back to the test-requesting physician. The process is designed to work within a timeframe of 72 hours from sample receipt to result release. Eight variants for (B) ROS1 and (C) RET are covered within the multiplexed assays. Adapted from Biodesix website with permission. Please click here to view a larger version of this figure.
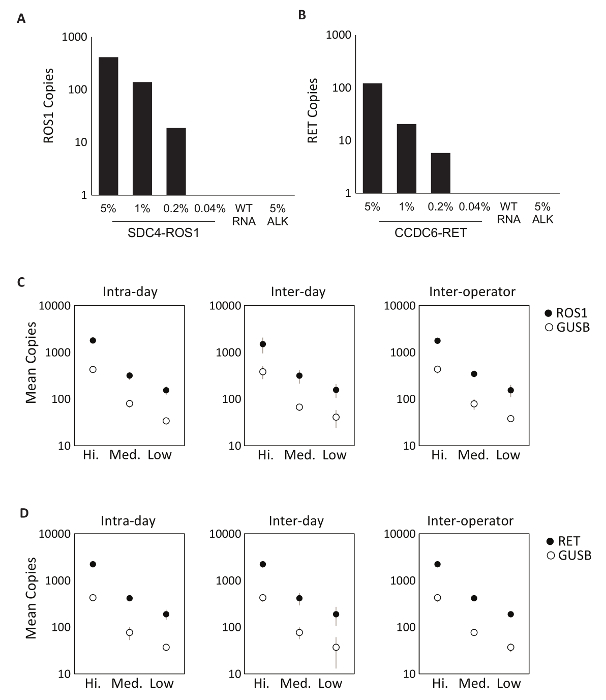
Figure 2: Analytic Validation. Cell-lines expressing (A) SDC4-ROS1 fusion and (B) CCDC6-RET fusion were diluted in a background of total human wild-type RNA (WT RNA). With each fusion variant, the limit of detection was established at 0.2% variant frequency using pre-defined criteria for each variant assay. All samples above this threshold also contained at least 21 copies of control gene. 5% EML4-ALK (ALK) standard in a background of wild-type RNA was tested to demonstrate assay specificity, which was confirmed by a negative result. Analytic multiplexed RNA standards were measured at high, medium, and low concentrations for (C) ROS1 and (D) RET. Precision was evaluated over three runs on the same day (Intra-day), three runs on three consecutive days (Inter-day), and with two independent operators (Inter-operator). The means of copy number and standard deviations are shown. Adapted from Biodesix website with permission. Please click here to view a larger version of this figure.
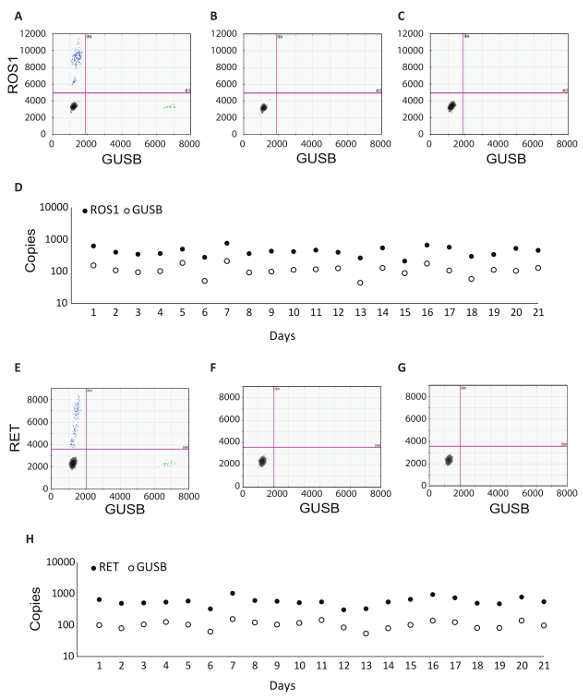
Figure 3: Batch Processing Control Examples and Robustness Data. 2D plot of the ROS1 multiplexed assay dPCR results for (A) positive control, (B) no reverse transcriptase control, and (C) no RNA template control. (D) Controls were run on 21 consecutive days (excluding weekends and holidays). Mean copy number +/- standard deviations for ROS1 positive control were 439 +/- 141. No reverse transcriptase and no template controls were also run on each day, and these were all negative (data not shown). 2D plot of the RET multiplexed assay dPCR results for (E) positive control, (F) no reverse transcriptase control and (G) no RNA template control. (H) Controls were run on 21 consecutive days (excluding weekends and holidays). Mean copies +/- standard deviations for RET positive control were 586 +/- 182. Not shown are no reverse transcriptase and no template controls that were also run on each day and were all negative. Adapted from Biodesix website with permission. Please click here to view a larger version of this figure.
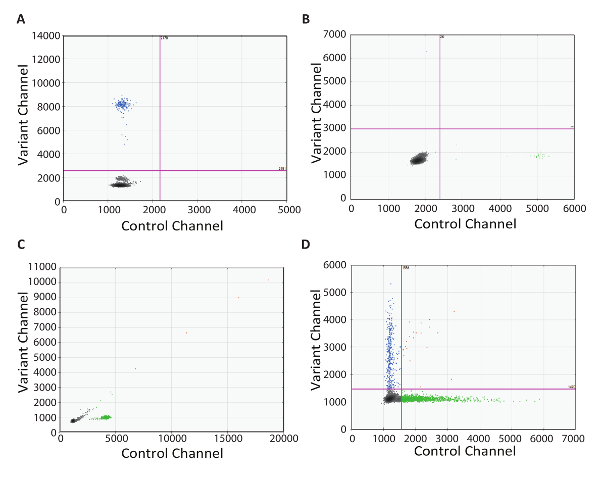
Figure 4: Troubleshooting RT-dPCR. 2D plots representing sub-optimal dPCR results obtained when there is (A) contamination within the no reverse transcriptase control, (B) contamination within the no RNA control, (C) shearing and coalescing of droplets, and (D) poorly optimized PCR conditions or PCR inhibition. Please click here to view a larger version of this figure.
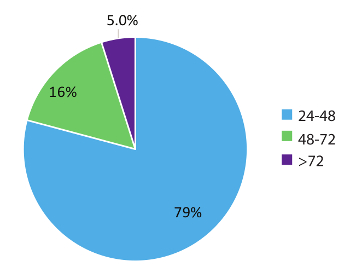
Figure 5: Turnaround time (TAT). TAT (in hours) was compiled for tests requesting an RNA variant (n = 984). Data excludes weekends, holidays, and samples held for >24 h due to incomplete clinical information on the laboratory Test Request Forms. Please click here to view a larger version of this figure.
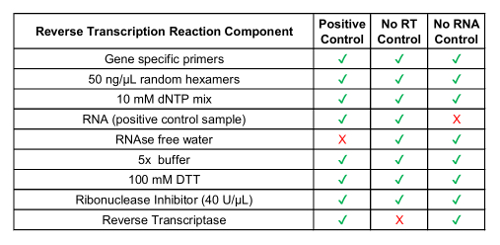
Table 1: Preparation of Reverse Transcription Reagents for Process Controls.
| Component | Volume |
| 2x dPCR supermix for probes (no 2’-deoxyuridine 5’-triphosphate) |
10 µL |
| 20x variant target primers/probes set (450 nmol/L primers, 250 nmol/L FAM probe) |
1 µL |
| 20x control target primers/probe set (450 nmol/L primers, 250 nmol/L HEX probe) |
1 µL |
| nuclease-free water | 1 µL |
| cDNA | 7 µL |
Table 2: Preparation of the master mix for dPCR.
| Cycling Step | Temperature | Time | # Cycles | Ramp Rate |
| Enzyme activation | 95 °C | 10 min | 1 | ~2 oC/s |
| Denaturation | 94 °C | 30 s | 40 | |
| Annealing/extension | 55 °C | 1 min | ||
| Enzyme deactivation | 98 °C | 10 min | 1 | |
| Hold (optional) | 4 °C | infinite | 1 | ~1 oC/s |
Table 3: Thermal Cycling Conditions.
