The application of 100 µM 4-AP to good-quality (undamaged) 450 µm-sized cortical brain slices from a juvenile VGAT-ChR2 mouse reliably induced recurrent ictal events (> 5 s) within 15 min (Figure 1Ai). The application of 100 µM 4-AP to slices of poor-quality resulted in bursting events or spiking activity (Figure 1Aii). On average, 40% of the slices from each dissected mouse brain successfully generated ictal events. Moreover, 83% (25/30) of the dissected mice resulted in at least one brain slice that successfully generated ictal events. In brain slices with spontaneously occurring ictal events, the application of a brief 30 ms light pulse on the brain slice reliably triggered an ictal event that was identical in morphology (Figure 1Aiii and 1Aiv). The same findings were made in brain slices from Thy1-ChR2 mice (Figure 1B). Thus, regardless of which neuronal-subpopulation was activated, any brief synchronizing event in the isolated cortical neural network led to the onset of an ictal event. These ictal events were comprised of a sentinel (preictal) spike (Figure 2Aii and 2Bii), tonic-like firing (Figure 2Aiii and 2Biii), clonic-like firing (Figure 2Aiv and 2Biv), and bursting activity toward the end (Figure 2Av and 2Bv); they were similar in nature to the electrographic signatures associated with clinical seizures33. Moreover, these juvenile mice were physiologically adult-like as the addition of 10 µM bumetanide (BUM), an NKCC1 blocker, had no effect on the resulting ictal events (Figure 2).
The in vitro 4-AP cortical slice model reliably generated consistent ictal events for ~1 h (Figure 1Ai), whereas the Zero-Mg2+ model typically generated ictal events for ~10 min before rapidly transforming into burst-like activity (Figure 3A). However, if a non-4-AP method of seizure induction is required, the Zero-Mg2+ model can be modified with the addition of 5 – 10 µM baclofen (a GABAB receptors agonist) to transform the bursting activity back into ictal events (Figure 3B). In general, methods of non-disinhibition to increase excitability (i.e., 4-AP or Zero-Mg2+ ACSF) reliably reproduced ictal events in cortical brain slices. In contrast, methods of disinhibition [i.e., bicuculline (BMI), a GABAA receptor antagonist] resulted in spiking activity reminiscent of interictal activity or bursting activity, rather than ictal events (Figure 4A). Similarly, acute seizure models prepared from 100 µM 4-AP-treated hippocampal slices generated interictal-like spiking activity or status epilepticus-like conditions in the CA3 (Figure 4B). The in vivo 4-AP cortical model correspondingly generated recurrent ictal events (> 5 s). Ictal events were observed in the superficial layer (2/3) within ~30 min of topically applying 1.5 mM 4-AP onto the exposed cortex of adult VGAT-ChR2 mice. The application of a brief 30 ms light pulse onto the exposed cortex reliably triggered ictal events that were morphologically similar to those spontaneously occurring (Figure 5).
The application of Zero-Mg2+ human ACSF with 100 µM 4-AP to 'non-epileptic' cortical brain slices (450 µm) from temporal lobe epilepsy patients reliably generated recurrent ictal events (> 5 s) within ~30 min (Figure 6Ai and 6Bi). Slices of poor quality generated either spiking activity or no activity (Figure 1Aii). The viability of brain slices was deemed 'good quality' when a brief electrical stimulus (100 µs, 30 – 300 µA) induced a robust, evoked response in the LFP at the beginning of the experiment. Once ictal events began to precipitate, the application of a brief puff (75 ms at 20 psi) of 100 mM GABA onto the brain slice reliably triggered ictal events that were identical in morphology to those occurring spontaneously (Figure 6Aii and 6Aiii). A lower concentration of GABA, 100 – 200 µM, will likely be effective as well for in vitro experiments34; however, a higher concentration of GABA, 100 mM, is recommended for in vivo experiments35. The same observations were reproduced when a brief puff of 200 µM glutamate was applied to human brain slices (Figure 6Bii and 6Biii). Thus, regardless of which post-synaptic receptors were activated, a brief synchronizing event in the isolated human cortical neural network reliably triggered an ictal event.
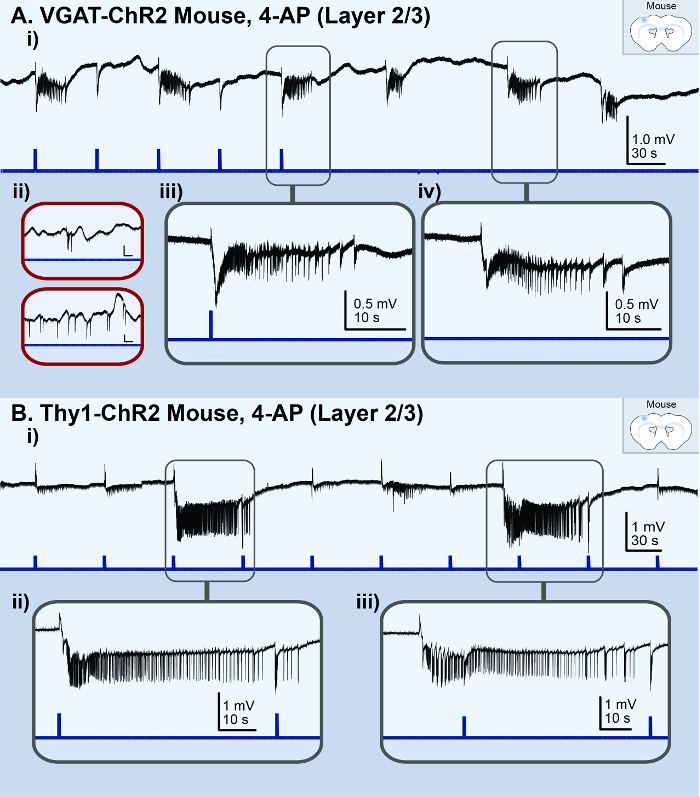
Figure 1: Acute in vitro 4-AP cortical seizure model. The black lines represent the local field potential (LFP) recording; the blue lines represent the light stimulus. (A) These panels are based on the results from a VGAT-ChR2 mouse model. They illustrate ictal events observed in the LFP recording from the superficial layer (2/3) of a high-quality cortical brain slice treated with 100 µM 4-AP. i) This panel shows an overview of the LFP recording. ii) These are examples of the LFP recording from poor-quality brain slices. The vertical scale bar is 0.4 mV, the horizontal scale bar is 20 s. iii) This is a zoomed-in view of a light-triggered ictal event. iv) This is a zoomed-in view of a spontaneous ictal event. (B) These panel are based on the results from a Thy1-ChR2 mouse model. They illustrate ictal events observed in the LFP recording from the superficial layer (2/3) of a cortical brain slice treated with 100 µM 4-AP. i) This panel shows an overview of the LFP recording. ii) This is a zoomed-in view of a light-triggered ictal event. iii) This is a zoomed-in view of a spontaneous ictal event. Please click here to view a larger version of this figure.
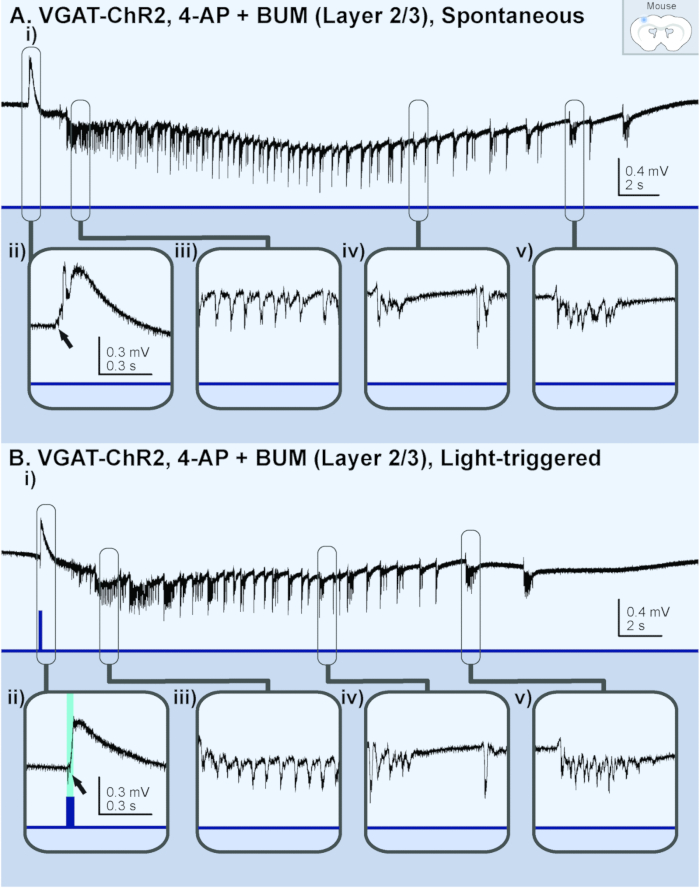
Figure 2: Ictal events generated in a brain slice (layer 2/3) from a juvenile (p13) VGAT-ChR2 mouse perfused with 4-AP and bumetanide (BUM). The black lines represent the local field potential (LFP) recording; the blue lines represent the light stimulus. (A) These panels show a spontaneous ictal event. i) This panel shows an overview of the entire ictal event. The following panels show ii) a sentinel spike, iii)tonic-like firing, iv) clonic-like firing, and v) bursting activity. (B) These panels show a light-triggered ictal event. i) This panel shows an overview of the entire ictal event. The following panels show ii) a light-triggered sentinel spike from the same slice recording, iii) tonic-like firing, iv) clonic-like firing, and v) bursting activity. Please click here to view a larger version of this figure.
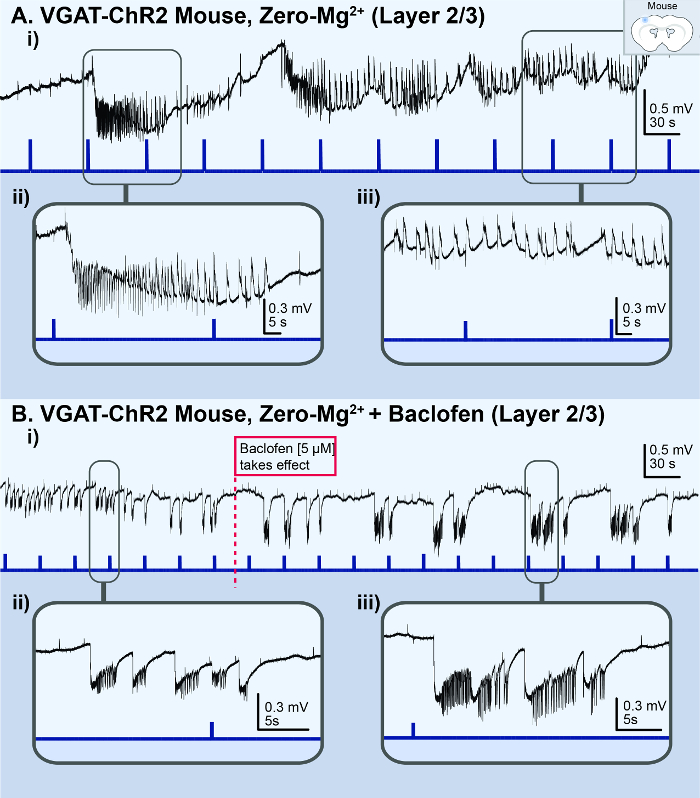
Figure 3: Acute in vitro Zero-Mg2+ cortical seizure model. The black lines represent the local field potential (LFP) recording; the blue lines represent the light stimulus. (A) These panels are based on the results from a VGAT-ChR2 mouse model. i) This panel illustrates the status epilepticus-like conditions observed in the LFP recording from the superficial layer (2/3) of a cortical brain slice treated with Zero-Mg2+ ACSF. ii) This is a zoomed-in view of a light-triggered ictal event. iii) This is a zoomed-in view of the status epilepticus-like bursting activity. (B) These panels show the same slice recording with the addition of baclofen. i) The application of 5 µM baclofen to the Zero-Mg2+ ACSF transforms the bursting activity back into distinct, recurrent ictal events. ii) This is a zoomed-in view of the bursting activity. iii) This is a zoomed-in view of the distinct ictal event. Please click here to view a larger version of this figure.
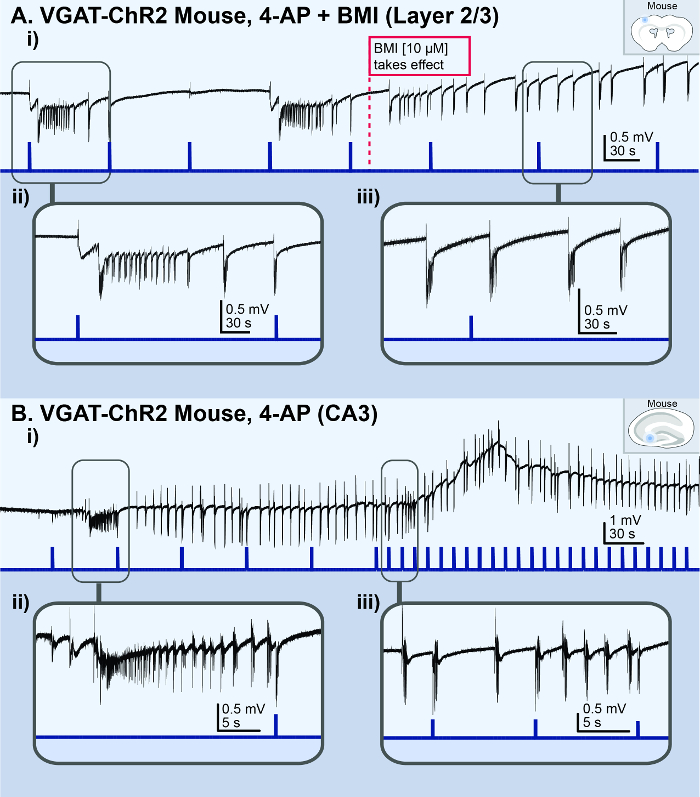
Figure 4: Acute in vitro bursting/spiking models. The black lines represent the local field potential (LFP) recording; the blue lines represent the light stimulus. (A) These panels show the results from a cortical slice from a VGAT-ChR2mouse, illustrating the bursting activity observed in the superficial layer (2/3) following the addition of 10 µM BMI to 100 µM 4AP. i) This is an overview of the LFP recording. The dotted red line indicates when the BMI took effect. ii) This is a zoomed-in view of a light-triggered ictal event. iii) This is a zoomed-in view of the spontaneous bursting activity. (B) These panels show the results from a hippocampal slice from a VGAT-ChR2 mouse, illustrating a status epilepticus-like event observed in the CA3 area following the application of 100 µM 4AP. i) This is an overview of the LFP recording. ii) This is a zoomed-in view of an ictal event. iii) This is a zoomed-in view of light-triggered and spontaneous bursting events. Please click here to view a larger version of this figure.
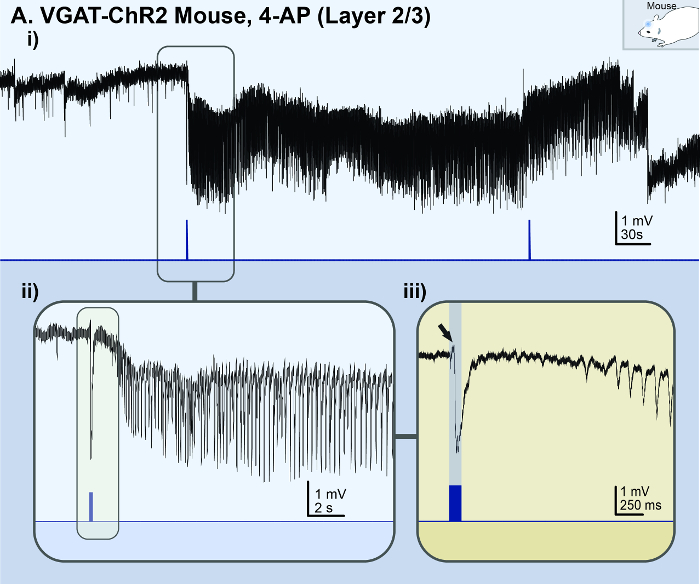
Figure 5: Acute in vivo 4-AP cortical seizure model. The black lines represent the local field potential (LFP) recording; the blue lines represent the light stimulus. (A) These panels show the results of an adult (p56) VGAT-ChR2 mouse model with 1.5 mM 4-AP topically applied to the exposed cortex. i) This panel illustrates a light-triggered ictal event observed in the superficial layer (2/3) of the somatosensory-motor area. ii) This is a zoomed-in view of the light-triggered ictal event from panel Ai. iii) This is a super zoomed-in view of the onset of the light-triggered ictal event (indicated by the black arrow). This figure is the unfiltered version of a figure from Chang et al.16. Please click here to view a larger version of this figure.
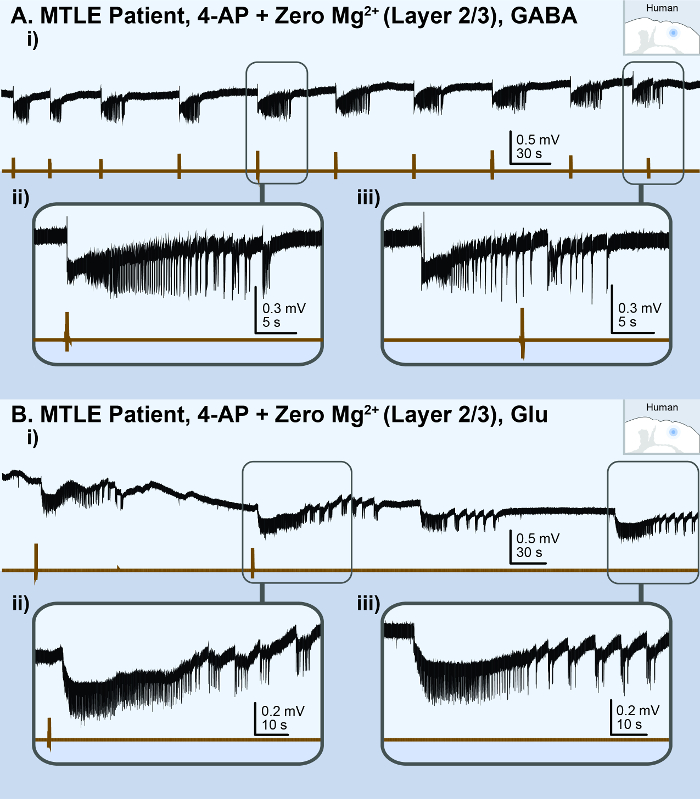
Figure 6: Acute in vitro human cortical seizure model. The black lines represent the local field potential (LFP) recording; the brown lines represent the picospritzer puff. (A) These panels show the results of a cortical brain slice from a medial temporal lobe epilepsy (MTLE) patient, illustrating the ictal events observed in the superficial layer (2/3) following a perfusion with 100 µM 4-AP and Zero-Mg2+ human ACSF. i) This is an overview of the LFP recording. The following panels show ii) a zoomed-in view of a 100 mM GABA puff-triggered ictal event and iii) a zoomed-in view of a spontaneous ictal event. (B) These panels show the results of a cortical brain slice from another MTLE patient, illustrating the ictal events observed in the superficial layer (2/3) following a perfusion with 100 µM 4-AP and Zero-Mg2+ human ACSF. i) This is an overview of the LFP recording. The following panels show ii) a zoomed-in view of a 200 µM glutamate puff-triggered ictal event and iii) a zoomed-in view of a spontaneous ictal event. Please click here to view a larger version of this figure.
| # | Reagent | Conc. [mM] | MW (g/mol) | 1L (g) | 2L (g) |
| 1 | Sucrose | 248 | 342.3 | 84.89 | 169.78 |
| 2 | Sodium Bicarbonate (NaHCO2) | 26 | 84.01 | 2.18 | 4.37 |
| 3 | Dextrose (D-glucose) | 10 | 180.16 | 1.8 | 3.6 |
| 4 | Potassium Chloride (KCl) | 2 | 74.55 | 0.15 | 0.3 |
| 5 | Magnesium Sulfate (MgSO4·7H2O) | 3 | 246.47 | 0.74 | 1.48 |
| 6 | Sodium phosphate monobasic monohydrate (H2NaPO4·H2O) | 1.25 | 137.99 | 0.17 | 0.34 |
| 7 | Calcium Chloride (CaCl2·2H2O) | 1 | 147.01 | 0.15 | 0.29 |
Table 1: Recipe for dissection solution. These are instructions to make 1 L or 2 L volumes. MW = the molecular weight of the solute.
| # | Reagent | Conc. [mM] | MW (g/mol) | 2L (g) | 4L (g) |
| 1 | Sodium Chloride (NaCl) | 123 | 58.4 | 14.37 | 28.73 |
| 2 | Sodium Bicarbonate (NaHCO2) | 26 | 84.01 | 4.37 | 8.74 |
| 3 | Dextrose (D-glucose) | 10 | 180.16 | 3.6 | 7.21 |
| 4 | Potassium Chloride (KCl) | 4 | 74.55 | 0.6 | 1.19 |
| 5 | Magnesium Sulfate (MgSO4·H2O) | 1.3 | 246.47 | 0.64 | 1.28 |
| 6 | Sodium phosphate monobasic monohydrate (HNaPO4·H2O) | 1.2 | 137.99 | 0.33 | 0.66 |
| 7 | Calcium Chloride (CaCl2·2H2O) | 1.5 | 147.01 | 0.44 | 0.88 |
Table 2: Recipe for rodent artificial cerebral spinal fluid (ACSF). These are instructions to make 2 L or 4 L volumes. MW = the molecular weight of the solute.
| # | Reagent | Conc. [mM] | MW (g/mol) | 2L (g) | 4L (g) |
| 1 | Sodium Chloride (NaCl) | 123 | 58.4 | 14.38 | 28.75 |
| 2 | Sodium Bicarbonate (NaHCO2) | 25.2 | 84.01 | 4.23 | 8.46 |
| 3 | Dextrose (D-glucose) | 10 | 180.16 | 3.6 | 7.21 |
| 4 | Potassium Chloride (KCl) | 4 | 74.55 | 0.6 | 1.19 |
| 5 | Magnesium Sulfate (MgSO4·H2O) | 1 | 246.47 | 0.49 | 0.99 |
| 6 | Sodium phosphate monobasic monohydrate (HNaPO4·H2O) | 1.2 | 137.99 | 0.33 | 0.66 |
| 7 | Calcium Chloride (CaCl2·2H2O) | 1 | 147.01 | 0.29 | 0.59 |
Table 3: Recipe for human artificial cerebral spinal fluid (human ACSF). These are instructions to make 2 L or 4 L volumes. MW = the molecular weight of the solute.
| # | Reagent | Conc. [mM] | MW (g/mol) | 2L (g) | 4L (g) |
| 1 | Sodium Chloride (NaCl) | 123 | 58.4 | 14.37 | 28.73 |
| 2 | Sodium Bicarbonate (NaHCO2) | 26 | 84.01 | 4.37 | 8.74 |
| 3 | Dextrose (D-glucose) | 10 | 180.16 | 3.6 | 7.21 |
| 4 | Potassium Chloride (KCl) | 4 | 74.55 | 0.6 | 1.19 |
| 5 | Magnesium Sulfate (MgSO4·H2O) | Nominally Free | 246.47 | 0 | 0 |
| 6 | Sodium phosphate monobasic monohydrate (HNaPO4·H2O) | 1.2 | 137.99 | 0.33 | 0.66 |
| 7 | Calcium Chloride (CaCl2·2H2O) | 1.5 | 147.01 | 0.29 | 0.59 |
Table 4: Recipe for Zero-Mg2+ rodent artificial cerebral spinal fluid (Zero-Mg2+ ACSF). These are instructions to make 2 L or 4 L volumes. MW = the molecular weight of the solute.
| # | Reagent | Conc. [mM] | MW (g/mol) | 2L (g) | 4L (g) |
| 1 | Sodium Chloride (NaCl) | 123 | 58.4 | 14.38 | 28.75 |
| 2 | Sodium Bicarbonate (NaHCO2) | 25.2 | 84.01 | 4.23 | 8.46 |
| 3 | Dextrose (D-glucose) | 10 | 180.16 | 3.6 | 7.21 |
| 4 | Potassium Chloride (KCl) | 4 | 74.55 | 0.6 | 1.19 |
| 5 | Magnesium Sulfate (MgSO4·H2O) | Nominally Free | 246.47 | 0 | 0 |
| 6 | Sodium phosphate monobasic monohydrate (HNaPO4·H2O) | 1.2 | 137.99 | 0.33 | 0.66 |
| 7 | Calcium Chloride (CaCl2·2H2O) | 1 | 147.01 | 0.29 | 0.59 |
Table 5: Recipe for Zero-Mg2+ human artificial cerebral spinal fluid (Zero-Mg2+ human ACSF). These are instructions to make 2 L or 4 L volumes; MW = the molecular weight of the solute.
