The purpose of these representative results is to illustrate the feasibility of the protocol.
Patients
In total, 663 patients were admitted to the ICU between 14-05-2018 and 15-08-2018. Of these, 208 patients were eligible for inclusion (reasons for exclusion are displayed in Figure 4). A number of 49 patients were excluded as there was no possibility to perform the CCUS due to ongoing resuscitation efforts. Seven patients refused to participate (no informed consent) and in four patients CCUS was impossible, e.g., due to prone positioning for mechanical ventilation or vacuum assisted closure of large wounds, resulting in 138 included patients with data for analysis.
CCUS validation and image quality
Extensive validation of cardiac imaging is planned. Renal ultrasonography validation has been initiated. So far, images of 21 patients (15%) were validated. In 18 patients (86%) images appeared of sufficient quality. All reasons for disapproval of images were listed and returned for feedback to the researcher who performed the ultrasonography. The name of the researcher who performed the ultrasonography is recorded to be able to asses inter- and intra-observer variability using the Intraclass Correlation Coefficient (ICC). Exact statistical methods will be described in our statistical analysis plan, as was done in the SICS-I12.
Example case: Patient X, middle aged female
Patient X was admitted after she was found with impaired consciousness and low blood pressure. All obtained measurements are shown in Table 1. All variables were obtained within the required time set without missing data, illustrating the possible feasibility of this protocol. Within 3 hours after admission the first clinical examination was performed. During this examination the patient was sedated, intubated and needed vasopressor treatment. The second clinical examination was performed ten hours later and showed stable vitals after 700 mL of fluid infusion. Vasopressors were reduced. CCUS and biochemical analysis showed normal cardiac, IVC and renal function (Figure 5, Figure 6 and Figure 7). At T3, two days later, the vasopressors were stopped but cumulative positive fluid balance had risen to 6 liters, accompanied by an increased CO, wider IVC and diminished renal perfusion and function reflected by increased serum creatinine. At T4, 5 days after admission, fluid balance and serum creatinine had risen even further, where the patient developed stage 3 AKI. The patient died 2 days later due to multi organ failure with unclear origin, at 7 days after admission.
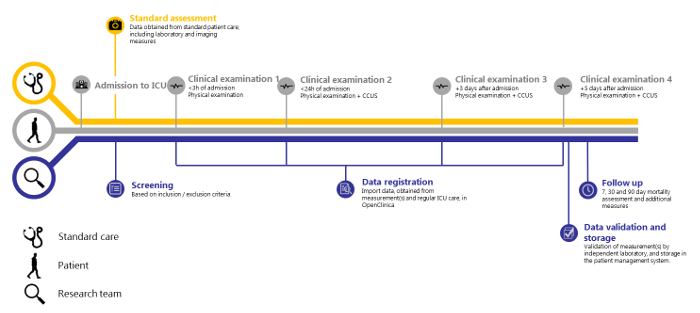
Figure 1: SICS-II study overview. Timeline of the SICS-II study from patient admission to Intensive Care to the final step of data registration. Please click here to view a larger version of this figure.
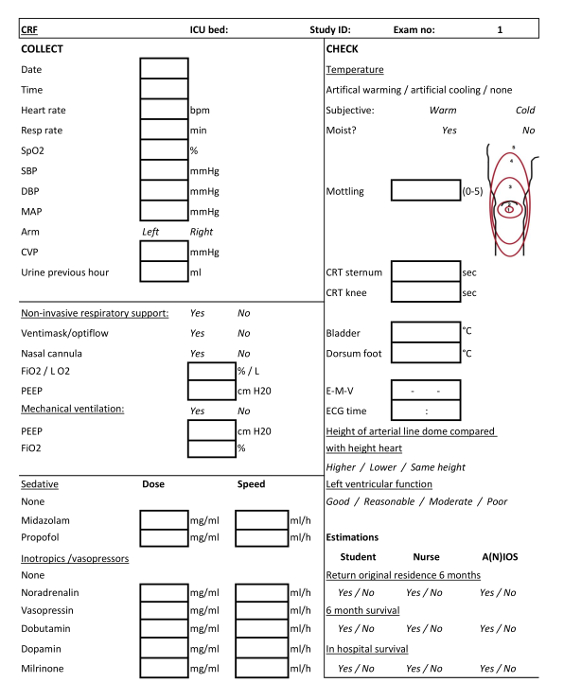
Figure 2: Case Report Form (CRF) for clinical examination 1. CRF to be filled by the ICU team students or student-researchers when conducting the first clinical examination. Please click here to view a larger version of this figure.
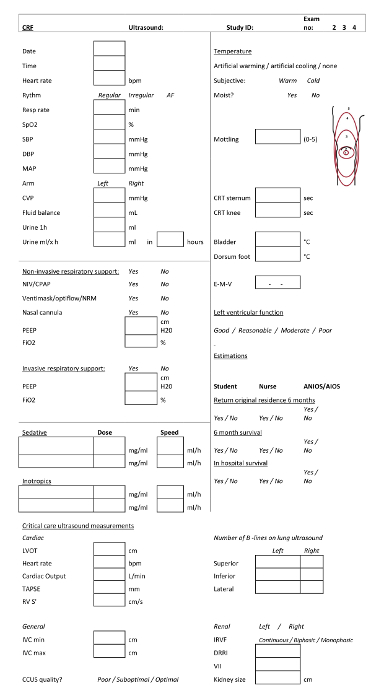
Figure 3: Case Report Form (CRF) for clinical examinations 2, 3 and 4. CRF to be filled by the ICU team students or student-researchers when conducting the second, third and fourth clinical examinations. Please click here to view a larger version of this figure.
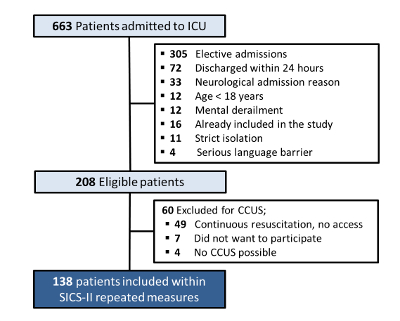
Figure 4: SICS-II patient inclusion and exclusion chart. Flowchart describing the criteria for patient inclusion and exclusion in the SICS-II study until 15-08-2018. Please click here to view a larger version of this figure.
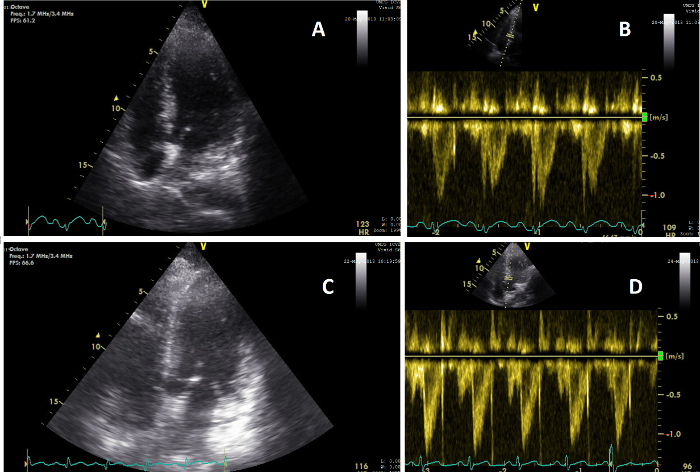
Figure 5: Apical views showing change in cardiac function. (A) Image of the heart on an AP4CH view during CCUS conducted during clinical examination 2 (T=2); (B) Image of the heart VTI pulse wave signal on T=2, showing a CO of 5.6 L/min; (C) Image of the heart on an AP5CH view during CCUS conducted during clinical examination 3 (T=3); (D) Image of the heart VTI pulse wave signal on T=3, showing a CO of 8.3 L/min. Please click here to view a larger version of this figure.
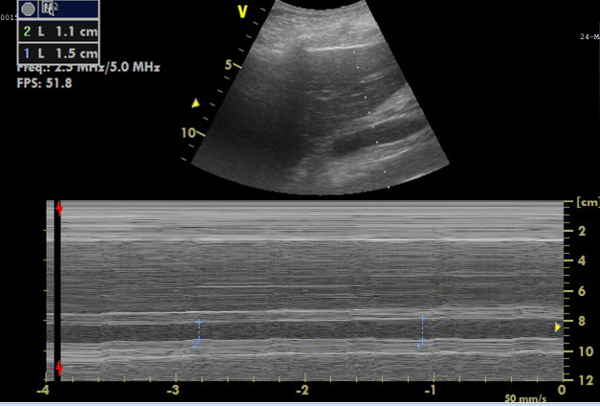
Figure 6: M-mode image of the inferior vena cava (IVC) for diameter measurements. Image showing, on top, the IVC in real-time, and, below, the M-mode image representing the IVC diameter changes, from which the collapsibility can be calculated. Please click here to view a larger version of this figure.
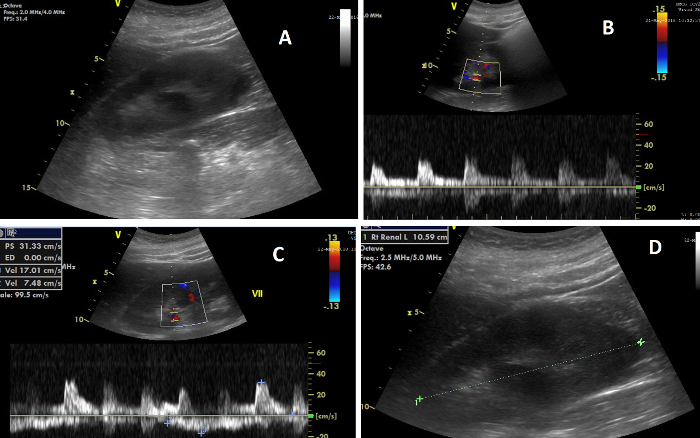
Figure 7: The various elements of renal ultrasonography. (A) Image of the right kidney during CCUS; (B) Image showing, on top, the Doppler flow in the renal arteries, and, below, the flow wave from which the renal resistive index is calculated; (C) Image showing, on top, the Doppler flow in the renal veins, and, below, the flow wave from which the venous impedance index is calculated; (D) Image illustrating the measurement of renal length. Please click here to view a larger version of this figure.
| Variable | T1 Day 1, at 00:38 |
T2 Day 1, at 10:53 |
T3 Day 3, at 10:14 |
T4 Day 5, at 10:20 |
| Heart rate (bpm) | 110 | 124 | 122 | 98 |
| Respiratory rate (breaths per min) | 24 | 15 | 26 | 12 |
| Systolic blood pressure (mmhg) | 100 | 115 | 130 | 118 |
| Diastolic blood pressure (mmhg) | 61 | 69 | 66 | 65 |
| Mean arterial pressure (mmhg) | 73 | 80 | 84 | 81 |
| Cumulative fluid balance (mL) | 0 | 704 | 7272 | 12338 |
| Mechanical ventilation | PEEP 5, FiO2 40% | PEEP 5, FiO2 40% | PEEP 5, FiO2 30% | PEEP 5, FiO2 30% |
| CRT sternum (seconds) | 1.5 | 2 | 4 | 3 |
| Central temperature (◦ C) | 37.6 | 37.5 | 38.0 | 37.4 |
| Urinary output previous hour (mL) | 117 | 60 | 0 | 10 |
| Administered inotropic agents | Noradrenaline 0.1 mg/ml 3.0 ml/h |
Noradrenaline 0.1 mg/ml 1.0 ml/h |
none | none |
| Administered sedative agents | Propofol 20 mg/ml 5.0 ml/h |
none | none | none |
| APACHE IV score | 92 | 88 | 87 | 90 |
| SOFA score | 8 | 8 | 5 | 8 |
| LVOT (cm) | N.A. | 2.4 | 2.4 | 2.4 |
| Cardiac output (L/min) | N.A. | 5.6 | 8.34 | 9.89 |
| TAPSE (mm) | N.A. | 25 | 26 | 21 |
| RV S’ (cm/s) | N.A. | 14 | 15 | 12 |
| IVC inspiratory diameter (cm) | N.A. | 1.14 | 1.24 | 1.10 |
| IVC expiratory diameter (cm) | N.A. | 1.27 | 1.38 | 1.50 |
| Kerley B lines (total) | N.A. | 6 | 2 | 4 |
| Renal length (cm) | N.A. | 10.59 | N.A. | N.A. |
| Intrarenal venous flow pattern | N.A. | Continuous | Continuous | Continuous |
| Doppler Renal RI | N.A. | 0.61 | 0.75 | 0.70 |
| VII | N.A. | 0.33 | 0.56 | 0.68 |
Table 1: A random SICS-II patient. Patient X, middle aged female admitted to the ICU after being found with impaired consciousness. Abbreviations: bpm = beats per minute, CRT = capillary refill time, LVOT = left ventricular outflow tract, TAPSE = tricuspid annular plane systolic excursion, RV S' = right ventricular systolic excursion, IVC = inferior vena cava, RRI = Renal resistive index, VII = venous impedance index, N.A. = not applicable.
| Variable | Unit | Source | Obtained at |
| Lactate | mmol/L | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| Chloride | mmol/L | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| pH | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 ho difference | |
| PCO2 | kPa | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| PaO2 | kPa | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| HCO3– | mmol/L | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| Hemoglobin | mmol/L | Arterial blood gas analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| Leukocytes | 10 x 10-9/L | Serum analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| Trombocytes | 10 x 10-9/L | Serum analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| HS Troponine | ng/L | Serum analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| ASAT | U/L | Serum analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| ALAT | U/L | Serum analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| Total bilirubin | uoml/L | Serum analysis | From standard care, as close as possible too each clinical examination, max 12 h difference |
| Creatinine | umol/L | Serum analysis | All measurements from start of ICU admission |
| Urine volume | ml | Urine collection of 24 h | All measurements from start of ICU admission |
| Creatinine | mmol/24 h | Urine analysis | All measurements from start of ICU admission |
Table 2: List of biochemical variables obtained. All patient biochemical variables collected during the study are listed here.
