The Ventilatory Parameters and Heart Rate
Based on the data (Figure 5), the NB and DB patterns were analyzed statistically (Figure 6 and Table 1). The f, VT and Te were found to have a significant interaction (p<0.05, respectively). A significant decrease in the f was found for both the NB and DB patterns during deep breathing compared to the initial rest phases (p<0.05, respectively), and, during deep breathing with the NB pattern, the f decreased to a greater extent compared to that for the DB pattern (Figure 6 and Table 1). The VT and Te revealed a significant increase during deep breathing compared to the initial rest phases for the NB and DB patterns, and, those for both deep breathing with the NB pattern were greater compared to those for the DB pattern (Figure 6). All of the parameters except VE and HR revealed main effect for the "phase" factor (Table 1).
A reduction in the work of breathing was reflected in a decrease in VO2, and, during deep breathing with the NB and DB patterns, the VO2 decreased with reduced work of breathing (Table 1). The improvement in ventilatory efficiency is reflected in an increase in VT and a decrease in f or VE. Deep breathing with the NB pattern was superior in ventilatory efficiency compared to that with the DB pattern. Generally, the relationship between VE and alveolar ventilation (VA) is calculated by the formula: VE= VT × f and VA = (VT– anatomic dead space) × f. Assuming that VE is a constant, a decreased respiratory rate and an increased VT indicate an improvement in VA. As VE yielded no significant interaction and main effect following 2-way ANOVA (Table 1), VE for deep breathing with both breathing patterns appeared to be equal. The respiratory rate during deep breathing with the NB pattern was significantly smaller compared to the DB pattern, but, for VT during deep breathing, it was significantly greater compared to that for the DB pattern (Figure 6 and Table 1). In other words, the alveolar ventilation or gas exchange during deep breathing with the NB pattern appears more efficient than for that during deep breathing with the DB pattern.
Breathing Patterns and Participants' Preference
Shown is the result of the visual assessment for thoracoabdominal movement during deep breathing with two methods of instructions (Table 2). For the NB pattern,The majority of the participants presented an upper costal or thoracoabdominal movement. During deep breathing with the DB pattern, all but one participant showed a thoracoabdominal or diaphragmatic movement. This result shows that the participants were able to carry out deep breathing as instructed. Thirteen out of the 15 participants expressed that they found the NB pattern easier to carry out than the DB pattern.
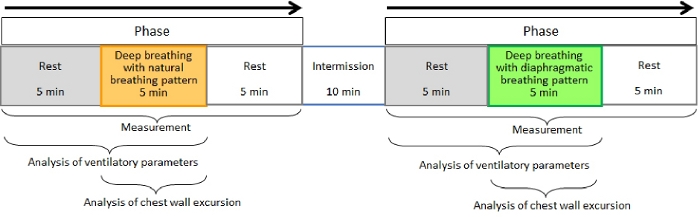
Figure 1. Flow chart for the protocol. Please click here to view a larger version of this figure.
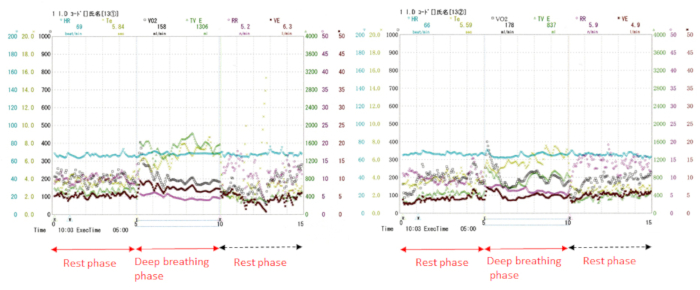
Figure 2. Ventilatory parameters as were seen displayed on the screen.
Left, Natural breathing pattern; Right, Diaphragmatic breathing pattern. Display shows a sample of individual data for each of the breath-by-breath samples for the ventilatory parameters and heart rate. Please click here to view a larger version of this figure.
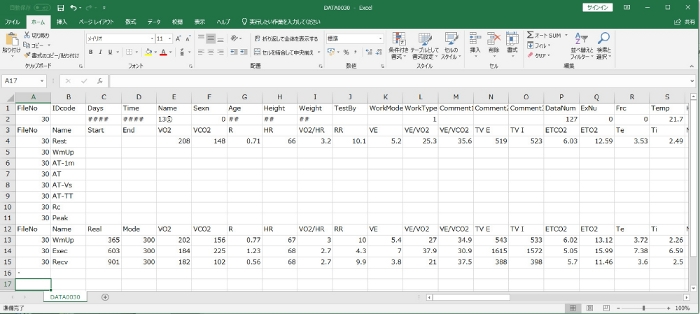
Figure 3. CSV format for ventilatory parameters during deep breathing with a natural breathing pattern.
The spreadsheet shows a sample of ventilatory parameters and heart rate following measurement. Please click here to view a larger version of this figure.
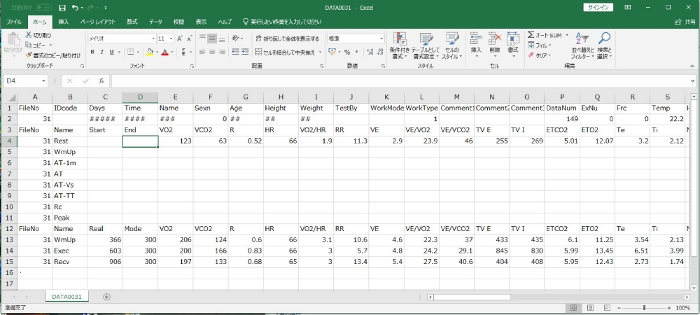
Figure 4. CSV format for ventilatory parameters during deep breathing with a diaphragmatic breathing pattern.
The spreadsheet shows a sample of ventilatory parameters and heart rate following measurement. Please click here to view a larger version of this figure.
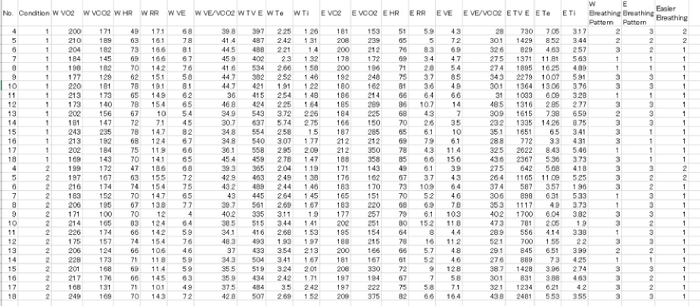
Figure 5. Raw data for all participants, which was converted from CSV data. Please click here to view a larger version of this figure.
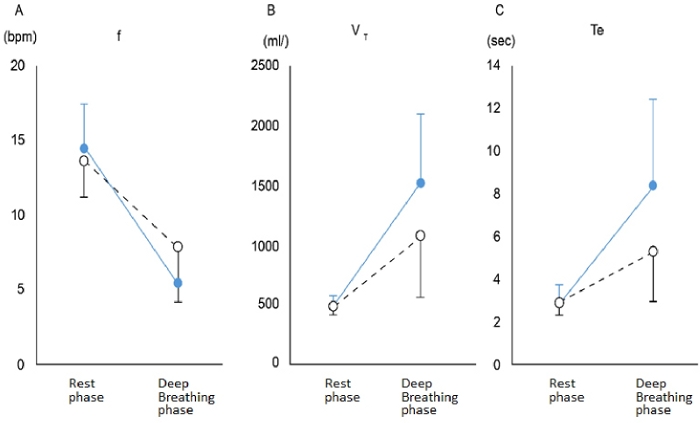
Figure 6. Significant interaction between ventilatory parameters.
Solid blue circle, deep breathing with natural breathing pattern; White circle, deep breathing with diaphragmatic breathing pattern. (A) shows the f, respiratory rate, (B) shows the VT, tidal volume, and (C) shows the Te, expiratory time. Please click here to view a larger version of this figure.
| Natural Breathing Pattern | Diaphragmatic Breathing Pattern | 2-way ANOVA | |||||
| Rest | Deep breathing | Rest | Deep breathing | Instruction | Phase | Interaction | |
| VO2 (L/min) | 0.20±0.02 | 0.19±0.01 | 0.20±0.02 | 0.19±0.01 | <0.01 | ||
| VCO2 (L/min) | 0.17±0.03 | 0.23±0.07 | 0.16±0.02 | 0.21±0.07 | <0.01 | ||
| VE (l/min) | 6.8±1.1 | 7.7±3.6 | 6.3±1.1 | 7.7±3.9 | |||
| f (/min) | 14.4±3.0 | 5.4±2.3* | 13.6±2.3 | 7.8±3.6†,§ | <0.01 | <0.05 | |
| VT (/ml) | 483±76 | 1507±579* | 464±61 | 1057±509†,§ | <0.05 | <0.01 | <0.05 |
| Te (s) | 2.79±0.92 | 8.37±4.00* | 2.82±0.53 | 5.25±2.31†,§ | <0.05 | <0.01 | <0.05 |
| Ti (s) | 1.63±0.43 | 4.51±1.70 | 1.69±0.33 | 3.67±1.08 | <0.01 | ||
| HR (bpm) | 69.1±7.6 | 71.7±8.9 | 68.5±7.6 | 70.1±8.5 | |||
Table 1. Comparison between the two breathing patterns. VO2, oxygen uptake; VCO2, carbon dioxide output; VE, minute ventilation; f, respiratory rate; VT, tidal volume; Te, expiratory time; Ti, inspiratory time; HR, heart rate; *, p<0.05 (Rest vs. Deep breathing during NB); †, p<0.05 (Rest vs. Deep breathing during DB); §, p<0.05 (NB vs. DB during Deep breathing). This table has been modified from one published in the Journal of Physical Therapy Science, 2018.
| Instruction | Upper costal | Thoracoabdominal | Diaphragmatic |
| Natural breathing pattern | 7 | 6 | 2 |
| Diaphragmatic breathing pattern | 1 | 8 | 6 |
Table 2. Result of the visual assessment for thoracoabdominal movement during deep breathing with two breathing patterns. This table has been modified from one published in the Journal of Physical Therapy Science, 2018.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}