In our study, 16 RP individuals and 14 healthy controls closely matched in age, sex, and education underwent resting-state fMRI scans. ReHo and FC methods were used to explore the intra-and intersynchronous neuronal activity in RP individuals. Significant differences in BCVA were observed between the right eye (P < 0.001) and the left eye (P < 0.001), but the difference in gender, age, or weight between the groups was not significant.
The RP and HCs show similar spatial distribution in the ReHo maps. However, the ReHo value of the visual area in RP patients was significantly lower than that in the control group (Figure 3A,B). Compared with HCs, the ReHo values of the RP individuals were significantly lower in the bilateral LGG/CPL (BA 17,18) compared to the HCs (Figure 4 and Table 1) (Two-tailed, voxel-level P < 0.01, GRF correction, cluster-level P < 0.05).
Compared with the HCs group, the RP group showed increased FC between the bilateral LGG/CPL and bilateral thalamus and decreased FC between the bilateral LGG/CPL and left postcentral (Figure 5 and Table 2).
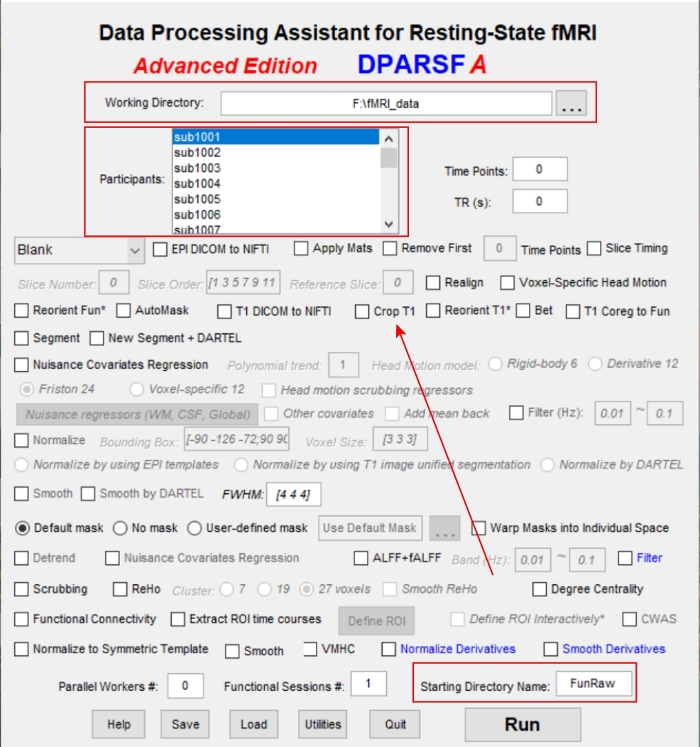
Figure 1: The operation interface of the DEPASFA toolbox. Please click here to view a larger version of this figure.
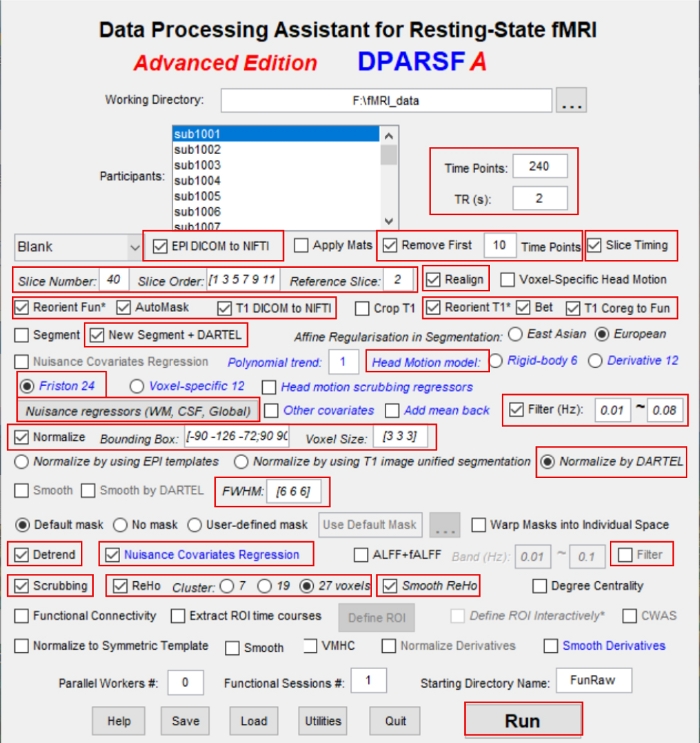
Figure 2: The operation interface of the DEPASFA toolbox with parameters entered. Please click here to view a larger version of this figure.
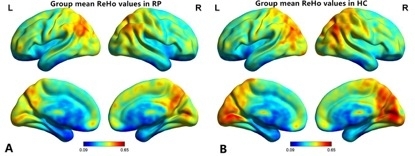
Figure 3: The distribution pattern of ReHo values in the RP and HC participants in the typical frequency band (0.01–0.08 Hz). Within-group means ReHo maps within the RP participants (A) and the HCs (B). ReHo = regional homogeneity; RP = retinitis pigmentosa; HC = health control; L = left hemisphere; R = right hemisphere. Please click here to view a larger version of this figure.
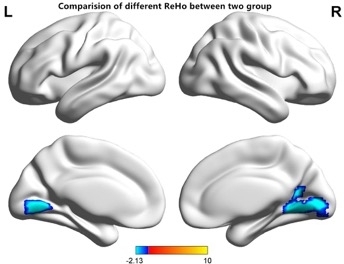
Figure 4: Comparisons of the ReHo values between the RP and HCs participants. There were significant regional differences in spontaneous activities between the two groups. ReHo values of RP participants were significantly lower in the bilateral LGG/CPL (BA 17,18) compared to those of HCs. The blue areas indicate lower ReHo values (two-tailed, voxel-level P < 0.01, GRF correction, cluster-level P < 0.05). GRF = Gaussian random field; LGG = lingual gyrus; CPL = cerebellum posterior lobe. Please click here to view a larger version of this figure.
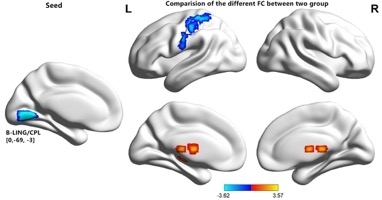
Figure 5: Comparisons of seed-based FC of the altered ReHo between the RP and HC groups. There were significant differences in seed-based FC activities between the two groups. The color-bars indicate the T-values. FC = functional connectivity; L = left hemisphere; R = right hemisphere; GRF = Gaussian random field; LGG = lingual gyrus; CPL = cerebellum posterior lobe. Please click here to view a larger version of this figure.
| Brain regions | BA | T-Peak scores | MNI coordinates | Cluster size (voxels) |
| (P-values) | (x, y, z) | |||
| Bilateral Lingual Gyrus/Cerebellum Posterior Lobe | 17,18 | -5.12, (<0.01) | 0, -69, -3 | 498 |
Table 1: Significant differences in the ReHo values between the two groups. The GRF theory was used to set the statistical threshold at the voxel level for multiple comparisons (P < 0.01). ReHo = regional homogeneity; BA = Brodmann area; RP = retinitis pigmentosa; HC = health control; MNI = Montreal Neurological Institute; GRF = Gaussian random field.
| Condition | Brain regions | BA | Peak T scores | MNI coordinates | Cluster size (voxels) |
| (x, y, z) | |||||
| ROI in bilateral LGG/CPL | |||||
| RP > HC | Left thalamus | – | 3.1668 | -21, -18, -3 | 70 |
| RP > HC | Right thalamus | – | 3.5733 | 18, -24, 21 | 219 |
| RP < HC | Left Postcentral | – | -3.6226 | -48, -21, 39 | 262 |
Table 2: Comparison of seed-based FC values of the altered ReHo regions between the two groups. The GRF correction method was used to set the statistical threshold at the voxel level for multiple comparisons (P < 0.01). FC = functional connectivity; ReHo = regional homogeneity; ROI = region of interest; LGG = Lingual Gyrus; CPL = cerebellum posterior lobe; BA = Brodmann area; RP = retinitis pigmentosa; HC = health control; MNI = Montreal Neurological Institute; GRF = Gaussian random field.
