EMG recording is a useful technique for measuring electrical activity produced by a skeletal muscle when activated by electrical stimulation of its nerve or spontaneous firing of its motor units. Monitoring EMG signals can be used for assessment of neuromuscular transmission and muscle biomechanics1. EMG recording also plays an important role in characterizing the quality and magnitude of muscle reinnervation following nerve injury2,3,4,5. However, multiple EMG recordings over the entire period of reinnervation cannot be achieved by an invasive approach. Therefore, implantable devices have been designed and developed for repeated, chronic stimulation and recording in neuromuscular systems6,7,8,9,10,11,12,13. The aim of this paper is to describe a protocol for the manufacturing and implantation of a stable system for obtaining reliable chronological EMG data from the larynx.
This system is applied here to the study of laryngeal muscle reinnervation. A brief overview of the larynx is provided for orientation (Figure 1). A precise coordination between sensory and motor components is essential for proper muscular movement during respiration, voicing, and airway protection. The PCA muscle, located in the posterior larynx, is the sole abductor of the vocal fold. This muscle is spontaneously activated during inspiration to increase glottal area for inhalation. The TA-LCA complex is the major adductor of the vocal fold. Activation of this muscle complex along with another adductor (i.e., the interarytenoid muscle) medialize the fold for vibration and sound production and close the fold for airway protection during swallowing.
Additionally, motor neuron fibers innervate both abductor and adductor muscles in the RLN. The abductor and adductor muscles can be distinguished based on motor unit composition14,15. The PCA muscle exhibits increased firing during hypercapnic and/or hypoxic conditions16 due to the presence of inspiratory motor units. In contrast, reflex glottic closure (RGC) motor units, which close the glottis reflexively through activation of sensory receptors within the laryngeal mucosa, is present in the TA-LCA muscle complex. The internal branch of the superior laryngeal nerve (SLN) carries the afferent fibers of sensory receptors in the larynx17. Although voicing is primarily an adductor function, both abductor and adductor motor units are involved in this highly evolved laryngeal behavior.

Figure 1: Anatomy of the larynx. The components of this implantable system are also displayed. SLN = superior laryngeal nerve; RLN = recurrent laryngeal nerve; PCA = posterior cricoarytenoid muscle; TA-LCA = thyroarytenoid–lateral cricoarytenoid muscle complex; DBS = deep brain stimulation. This figure has been reproduced with permission from Wiley27. Please click here to view a larger version of this figure.
Injury to the RLN can result in vocal fold paralysis (VFP), which compromises both abducting and adducting functions due to laryngeal muscle denervation14,18,19. Subsequently, regeneration of RLN nerve fibers and reinnervation of muscles commonly occurs. However, reinnervation is a random process and results in misdirected, inappropriate muscle reconnection in most cases. This is referred to as synkinesis, in which spontaneous activation of abductor and adductor antagonists is faulty and produces ineffective or even paradoxical movement of the vocal folds14,19,20,21. With synkinesis, the critical function that is lost is vocal fold abduction, resulting in inadequate ventilation. Although there are ongoing attempts to treat laryngeal synkinesis by either 1) blocking glottic closure with Botox22,23 or 2) electrically stimulating the glottic opening with an implantable pacemaker24,25, there is no clinical intervention that reliably prevents synkinesis26. However, there is evidence that electrical conditioning of the PCA muscle during reinnervation at a low frequency promotes appropriate neuromuscular reconnection and minimizes synkinesis from happening. Studies are currently being conducted to elucidate the underlying mechanisms2.
The focus of this paper is to describe a simple and inexpensive implantable system for chronic nerve stimulation and EMG recording. This system can be used to investigate the effects of low frequency electrical conditioning of the PCA muscle on the specificity of its subsequent reinnervation. EMG signals obtained by this system can reflect the quality and quantity of laryngeal muscle reinnervation over time.
Examples of the components are shown in Figure 2. From left to right in Figure 2A are the nerve stimulus cuff, TA-LCA recording electrode, PCA recording electrode, and skin interface receptacle, respectively. The relative size of these components can be appreciated. The skin receptacle (Figure 2B) has two rows of holes into which the female pins at the end of each coiled wire (Figure 2D) are inserted. They are inserted opposite the faceplate (arrow) during the implantation surgery. The receptacle has a polyester skirt (Figure 2C) attached to its connector sidewalls. This skirt is designed to anchor the receptacle in position by connective tissue infiltration. Each Teflon-coated stainless-steel EMG lead (Figure 2E) is deinsulated (5 mm) at the tip to form a hook-shaped electrode for muscle recording. The stimulation cuff has two electrodes threaded against the inner cuff wall. They are separated by a distance of 2 mm (Figure 2F) and form a “V” shape (Figure 2G) to ensure current delivery across the nerve.
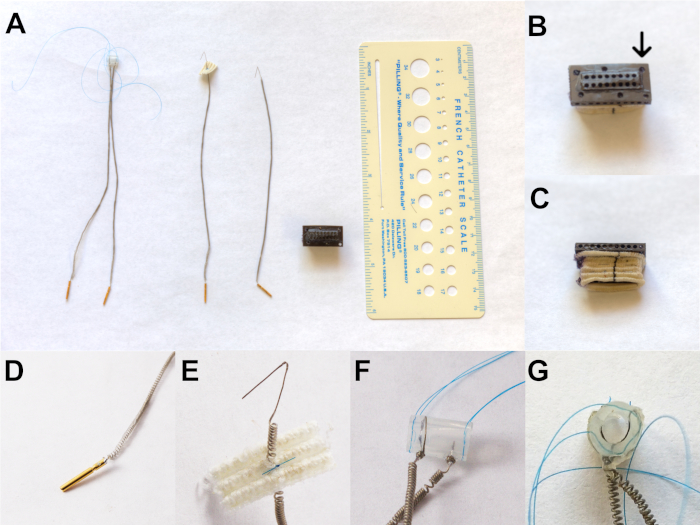
Figure 2: Components of the implant system. (A) From left to right is the nerve stimulus cuff, TA-LCA recording electrode, PCA recording electrode, and skin interface receptacle, respectively. (B) The skin receptacle showing two rows of holes. (C) The receptacle showing a polyester skirt attached to its connector sidewalls. (D) Coiled wire containing female pins to be inserted into B. (E) Teflon-coated stainless-steel EMG lead is deinsulated (5 mm) at the tip to form a hook-shaped electrode for muscle recording. (F) The stimulation cuff has two electrodes threaded against the inner cuff wall, which are separated by 2 mm. (G) “V” shape formation of electrodes to ensure current delivery across the nerve. This figure has been modified with permission27. Please click here to view a larger version of this figure.
Figure 3 shows the implanted skin receptacle and how the cable from external equipment is interfaced to the receptacles. It should be noted that dummy male pins (not shown) are inserted into the female pins of the receptacle to keep them free of debris between recording sessions.
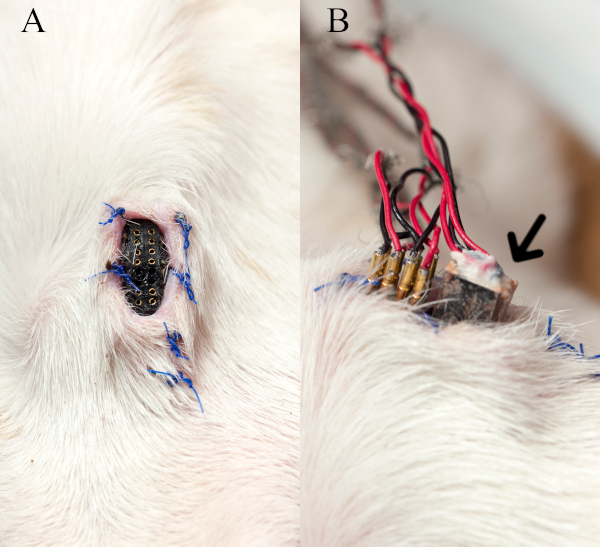
Figure 3: Skin receptacle and interface cable. (A) The implanted skin receptacle on the anterior neck without dummy male pins is shown. (B) The image depicts how the stimulus pins and EMG recording plug (arrow) of the cable from external equipment is interfaced to the receptacle during a nerve stimulation-EMG recording session. This figure has been modified with permission27. Please click here to view a larger version of this figure.
Figure 4 shows an EMG recording from one of the baseline sessions with the RLNs intact.
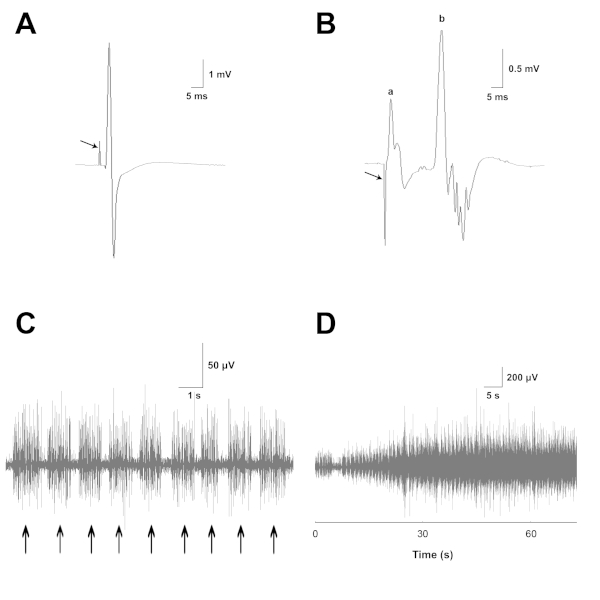
Figure 4: EMG recordings from laryngeal muscles with normal innervation. (A) Example recording from the PCA muscle where RLN stimulation produces a stimulus artifact (arrow) followed by a large evoked EMG potential. (B) Example recording of the TA-LCA muscle complex, in which SLN stimulation produces a stimulus artifact (arrow). Represented here is (a) a short latency monosynaptic muscle response and (b) a longer latency polysynaptic RGC response. (C) Bursts (arrows) of spontaneous EMG activity recorded from the PCA muscle during normal inspirations. (D) Increase of inspiratory EMG activity over the course of CO2 delivery. This figure has been modified with permission27. Please click here to view a larger version of this figure.
In a recording from the PCA muscle (Figure 4A), RLN stimulation produces a stimulus artifact (arrow) followed by a large evoked EMG potential. The maximum RLN-evoked responses provide a good index of the overall magnitude of normal innervation as well as the level of reinnervation following subsequent neurorrhaphy, irrespective of motor unit type. This is true because the RLN contains nerve fibers of both inspiratory and reflex glottic closure (RGC) motor units. RLN stimulation recruits both types of units. Evoked EMG motor unit activity is rectified and integrated over a 20 ms time period to obtain a quantitative measure of muscle innervation.
In a recording from the TA-LCA muscle complex (Figure 4B), SLN stimulation produces a stimulus artifact (arrow). This artifact is followed by a short-latency monosynaptic muscle response (a) and longer-latency polysynaptic RGC response (b). The potential (a) is a direct response from the cricothyroid muscle, because this muscle is innervated by the nearby external branch of the SLN. Stray activation of this branch commonly occurs during nerve cuff stimulation of the internal branch to activate the RGC response. The cricothyroid potential is recorded by the TA-LCA electrode, as this muscle is located near the complex. Previous studies have shown that the cricothyroid potential evoked by internal branch stimulation can be selectively abolished by sectioning the external branch of the SLN (Zealear, unpublished observations). The maximum SLN-evoked EMG responses reflect the magnitude of natural innervation of the TA-LCA complex through its RGC sensory-motor pathway. Prior to RLN neurorrhaphy, there is no RGC innervation of the PCA muscle, so no SLN potential should be detected from this muscle. Following nerve transection and repair, SLN-evoked potentials reflect the amount of correct RGC reinnervation of the TA-LCA complex and incorrect RGC reinnervation of the PCA muscle. RGC activity is quantified by rectification and integration over a 20 ms time period to capture the entire RGC waveform.
In (Figure 4C), bursts (arrows) of spontaneous EMG activity are recorded from the PCA muscle during normal inspirations. This inspiratory EMG activity increases over the course of CO2 delivery, as shown in (Figure 4D) at a slower sweep speed. Spontaneous PCA EMG activity provides a good estimate of the magnitude of normal innervation of this muscle by its original inspiratory motoneurons. There is no inspiratory innervation of the TA-LCA complex, so no inspiratory potentials should be detected from these muscles. This is because only inspiratory motor units are involved in abducting the vocal fold at maximal inspiratory effort in the anesthetized animal. Following nerve transection and repair, spontaneous inspiratory potentials reflect the magnitude of correct reinnervation of the PCA muscle and magnitude of incorrect reinnervation of the TA-LCA complex. Recordings of inspiratory EMG activity are amplified, rectified, and integrated over an 8 s time period.
