Sixteen male and female independent community-living older people with a mean age of 66.9 ± 5.0 years were enrolled in the study. The interventions and assessments were performed at the School of Physical Education of UNICAMP.
Statistical analysis was performed using Minitab 18 software. The Mann-Whitney test was used to compare the functional test results before and after training. P values smaller than 0.05 were considered significant. Delta was calculated as follows: (baseline values – post-training values) / baseline values x 100.
Significant differences between before and after training were determined using physical function tests to assess agility (Illinois test), lower limb strength and power (five times sit-to-stand), dynamic balance (TUG), gait (walking usual speed test), and static balance (one-leg stand).
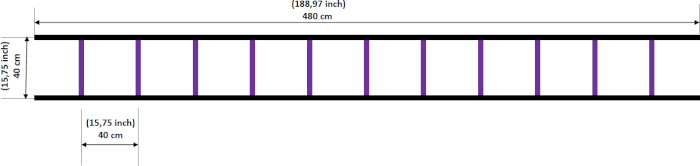
Figure 1: Agility ladder. The ladder had a length of 4.8 m and 12 rungs, forming 12 squares (40 cm x 40 cm). Please click here to view a larger version of this figure.

Figure 2: Walking usual speed test. Please click here to view a larger version of this figure.

Figure 3: Exercise set. Each 3-min set was composed of four 30 s subsets and a 15 s rest between subsets. Please click here to view a larger version of this figure.
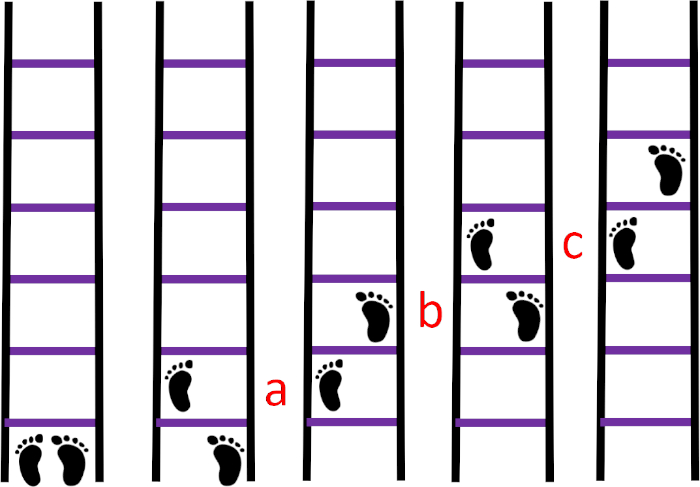
Figure 4: Sequence 1. (A) the left foot in the first square, (B) the right foot in the second square, (C) the left foot in the third square. Please click here to view a larger version of this figure.
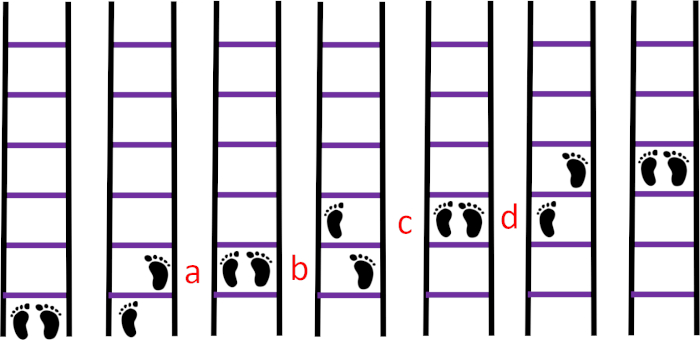
Figure 5: Sequence 2A. (A) The right foot in the first square, (B) the left foot in the first square, (C) the left foot in the second square, (D) the right foot in the second square. Please click here to view a larger version of this figure.
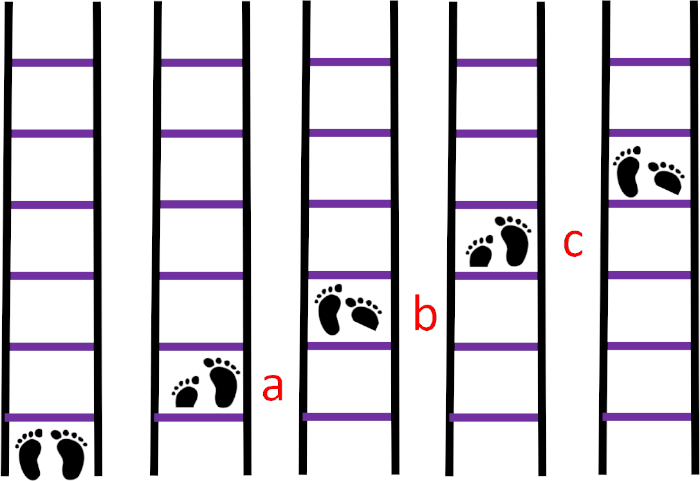
Figure 6: Sequence 2B. (A) The right foot in the first square and the toes of the left foot in the first square, (B) the left foot in the second square and the toes of the right foot in the second square, (C) the right foot in the third square and the toes of the left foot in the third square. Please click here to view a larger version of this figure.
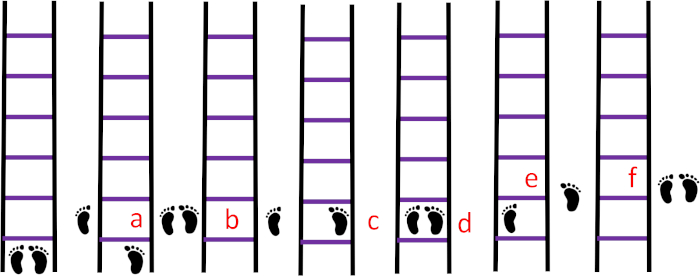
Figure 7: Sequence 3A. (A) The left foot outside the ladder to the left next to the first square, (B) the right foot outside the ladder next to the left foot, (C) the right foot in the first square, (D) the left foot in the first square, (E) the right foot outside the ladder to the right next to the first square, (F) the left foot next to the right foot. Please click here to view a larger version of this figure.
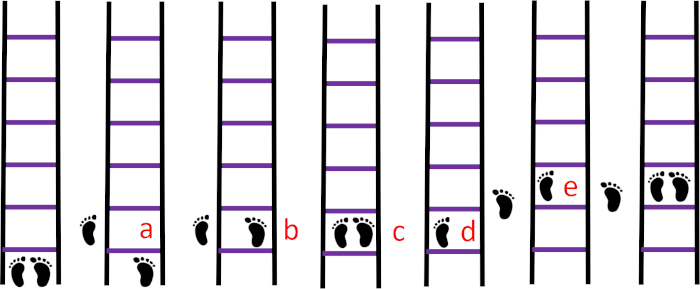
Figure 8: Sequence 3B. (A) The left foot outside the ladder to the left next to the first square, (B) the right foot in the first square, (C) the left foot next to the right foot, (D) the right foot outside of the ladder to the right next to the first square, (E) the left foot next to the right foot. Please click here to view a larger version of this figure.
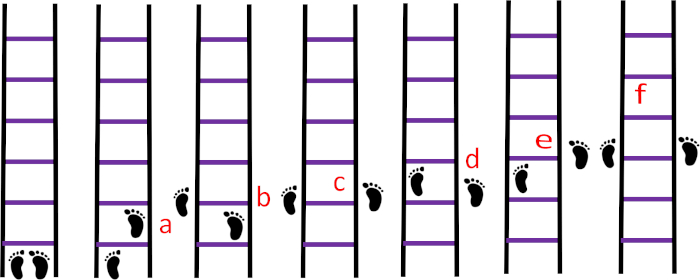
Figure 9: Sequence 4. (A) The right foot in the first square, (B) the left foot outside the ladder to the left next to the rung that separates the first and second squares, (C) the right foot outside the ladder to the right across from the left foot, (D) the left foot in the second square, (E) the right foot outside the ladder to the right next to the rung that separates the second and third squares, (F) the left foot outside the ladder across from the right foot. Please click here to view a larger version of this figure.
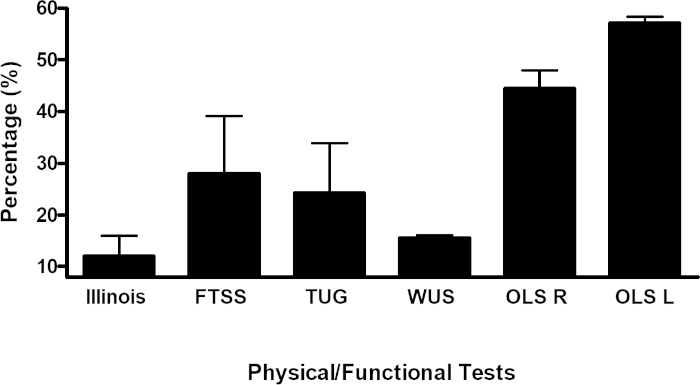
Figure 10: Delta values of the function test results. The percentage of training (delta) of each measurement was assessed over time. FTSS, five times sit-to-stand; WS, walking speed; TUG, timed up-and-go; OLS, one-leg stand using the right left (R) and left leg (L). Please click here to view a larger version of this figure.
| Tests | Pre | Post | P-Value |
| Illinois (s) | 35.9 ± 5.4 | 31.5 ± 4.5 | 0.02* |
| FTSS (s) | 10.7 ± 2.0 | 7.7 ± 1,1 | <0.01* |
| TUG (s) | 7.7 ± 1.2 | 5.8 ± 0.7 | <0.01* |
| WS (m/s) | 1.3 ± 0.1 | 1.5 ± 0,1 | <0.01* |
| OLS R (s) | 16.4 ± 10.4 | 23.7 ± 9.0 | 0.03* |
| OLS L (s) | 15.7 ± 8.5 | 24.6 ± 8.1 | 0.01* |
Table 1: Functional test results at baseline and post-training. Data are presented as means ± standard deviations and were considered significantly different at p < 0.05. *The Mann-Whitney test was used to compare differences between before and after training. FTSS, five times sit-to-stand; WS, walking speed; TUG, timed up-and-go; OLS, one-leg stand (OLS); R, right leg; L, left leg.
