Upper limb function is commonly impaired after stroke, and recovery of UL function is important for regaining independence in daily living activities1. Stroke rehabilitation trials are often aimed at improving UL recovery and outcomes after stroke. The majority of stroke rehabilitation research is conducted with patients at the chronic stage (>6 months poststroke), yet most rehabilitation occurs early after stroke2,3. More research needs to be conducted with patients soon after a stroke to build an evidence base for rehabilitation practice.
One of the greatest challenges when conducting research soon after the stroke is detecting the effects of the intervention against the background of recovery occurring during the initial weeks and months after the stroke. High intersubject variability in clinical presentation and recovery creates noise that can obscure the beneficial effects of interventions. Intervention and control groups are typically balanced on clinical measures of initial neurological impairment. However, these measures are often poor predictors of the patient's potential for subsequent recovery, particularly those with severe initial impairment4,5. This means that groups can be matched for baseline clinical measures and not matched for their recovery potential, which makes it more difficult to ascertain the intervention's effects. Biomarkers can address this challenge by identifying an individual patient's potential for motor recovery, so that groups can be accurately matched and stratified6,7,8. Biomarkers can also be used to select patients who are most likely to respond to the intervention's known or hypothesized mechanisms of action6.
The functional integrity of the corticospinal tract (CST) is a key biomarker that predicts recovery of UL function after stroke5,8,9,10,11,12. The CST conveys descending motor output from the primary motor cortex to the spinal cord and is essential for coordination and fine motor control. Patients with a functional CST after stroke are more likely to regain strength, coordination, and dexterity than patients without. A clinical assessment can be sufficient to confirm that the CST is functional in mildly impaired patients13,14,15. However, patients with more severe initial impairment may or may not have a functional CST, and a neurophysiological assessment using transcranial magnetic stimulation (TMS) is needed9,10,11,16,17.
TMS is a noninvasive and painless technique that can be used to test CST function18. The TMS coil delivers a magnetic stimulus over the primary motor cortex that generates a descending volley in the CST, eliciting a motor-evoked potential (MEP) in the muscles of the contralateral limb19. The presence of a MEP in the paretic arm or hand (MEP+) indicates a functional CST and is associated with greater potential for recovery of UL function. Patients who are MEP- are most likely to have worse UL recovery, with no return of coordinated and dexterous hand function4,6,9,12,16.
Testing all patients with TMS is impractical and unnecessary, as those with mild initial impairment most likely have a functional CST17. Therefore, a hierarchical approach is needed so that TMS is only used for patients with more severe initial impairment. The PREP2 algorithm was developed using a combination of clinical measures and TMS to evaluate CST function and predict likely UL outcome at 3 months poststroke (Figure 1)17. PREP2 starts at day 3 poststroke by testing the strength of shoulder abduction and finger extension in the paretic arm (SAFE score), using Medical Research Council grades. If the sum of these grades is 5 or more out of 10, it is "safe" to assume the patient is MEP+. These patients are expected to have a good or excellent UL outcome by 3 months poststroke, depending on their age17. These patients do not need TMS to determine MEP status, minimizing cost and unnecessary testing for the patient.
Patients with a SAFE score of less than 5 on day 3 poststroke require TMS to determine the functional integrity of their CST. If a MEP can be elicited from the paretic extensor carpi radialis (ECR) or first dorsal interosseus (FDI) muscles, the patient is MEP+ and is expected to recover fine motor control of the hand by 3 months poststroke. Approximately half of patients with a SAFE score less than 5 on day 3 poststroke are MEP+. Importantly, patients can have a SAFE score as low as zero and be MEP+. This illustrates the need for TMS in this subgroup of patients, as clinical assessment alone cannot distinguish between patients with and without a functional CST. Patients who are MEP- have significant CST damage. These patients are expected to have a limited or poor UL functional outcome depending on their overall stroke severity, measured with the National Institute of Health Stroke Scale (NIHSS) (Figure 1)17. These MEP- patients are not expected to regain coordinated and dexterous finger control and can be grouped together for research purposes.
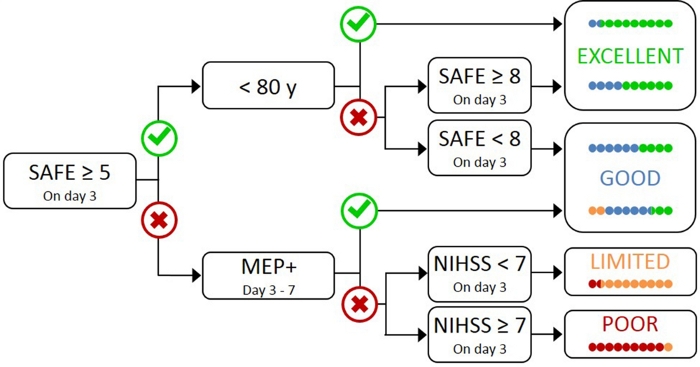
Figure 1: The PREP2 algorithm. SAFE = Shoulder Abduction, Finger Extension score, which is the sum of the Medical Research Council grades for each of these movements out of 5, for a total SAFE score out of 10. MEP+ = Motor Evoked Potentials can be elicited from the paretic extensor carpi radialis (ECR) and/or first dorsal interosseous (FDI) muscles of the paretic UL using transcranial magnetic stimulation. NIHSS = National Institutes of Health Stroke Scale. The algorithm predicts one of four possible UL functional outcomes at 3 months poststroke. Each prediction category is associated with a rehabilitation focus that can be used to tailor UL therapy2. The colored dots represent, proportionally, PREP2 algorithm accuracy. The dots are color-coded based on the outcome category actually achieved 3 months poststroke (Green = Excellent; Blue = Good; Orange = Limited; Red = Poor). Figure reproduced from Stinear et al.17. Please click here to view a larger version of this figure.
In clinical practice, PREP2 predicts one of four outcome categories that can be used to tailor rehabilitation for individual patients and help patients and families to understand what they can expect for their UL recovery. To date, PREP2 is the only externally validated UL prediction tool that combines clinical assessment and biomarker information in a decision tree17. It is also the only UL prediction tool with research on the effects of implementation in clinical practice20,21. PREP2 predictions are accurate for about 75% of patients, too optimistic for 17% and too pessimistic for 8% of patients at 3 months poststroke17. Accuracy is highest for MEP- patients (accurate for 90% of MEP- patients), highlighting the value of using TMS to identify these patients with severe damage to the descending motor pathways17. PREP2 remains correct for around 80% of patients at 2 years poststroke22. This supports the use of PREP2 to predict UL functional motor outcomes at 3 months and longer term. Information about delivering PREP2 predictions and using them in clinical practice is outside the scope of this methods paper, but detailed resources are available online23.
PREP2 provides researchers with a tool to select and stratify patients for clinical trials. This allows patients to be grouped not only according to baseline clinical characteristics, but also their neurobiological potential for UL recovery. Despite the mounting evidence for the use of TMS as a prognostic biomarker for UL recovery, lack of familiarity with TMS protocols in hospital settings with subacute stroke patients may be a barrier to its use in research. Therefore, this protocol aims to demonstrate how to use the SAFE score and TMS to evaluate CST function in patients in a hospital setting early after stroke.
The SAFE score and TMS can be used to ascertain the functional status of the CST within one week of stroke. Patients who have a SAFE score of at least 5 on day 3, or are MEP+ when tested with TMS, have a functional CST and are expected to regain at least some coordination and dexterity. Patients who are MEP- do not have a functional CST and therefore are likely to be limited to improvements in proximal arm movements and gross movements of the hand. The functional status of the CST can therefore be used to select patients for trials based on their capacity to recover dexterous hand function.
The PREP2 algorithm predicts UL functional outcomes by obtaining the SAFE score and MEP status using this protocol. The PREP2 algorithm has been developed and validated in patients aged 18 years or older, with ischemic or hemorrhagic stroke and new UL weakness, as described in detail elsewhere16,17,20. An important component of the PREP2 algorithm is determining MEP status with TMS for patients with a SAFE score less than 5. Patients must be assessed for suitability for the procedure. This includes completing a safety checklist that is subsequently reviewed and approved by the treating physician. The purpose of the checklist is to identify any contraindications or precautions for using TMS such as the presence of a cardiac pacemaker, seizures, brain surgery, and head injuries. Contraindications and precautions for TMS are well established and previously described in detail24.
A patient is considered to be MEP+ if a MEP is consistently present at an appropriate latency (20–30 ms for FDI, 15–25 ms for ECR) and with any peak-to-peak amplitude. The patient is MEP+ whether a MEP is elicited at rest or while attempting voluntary UL facilitation. The MEP only needs to be present in one muscle for the patient to be considered MEP+. This protocol differs from other protocols that may require a MEP to exceed 50 µV in peak-to-peak amplitude for at least 5 out of 10 traces. These other protocols are designed to establish the patient's rest motor threshold as a basis for further neurophysiological assessment. For prediction of UL recovery, the simple presence or absence of a MEP is a stronger predictor than MEP amplitude and identifying the rest motor threshold is not required8,9,16,25.
Figure 2, Figure 3, and Figure 4 provide examples of EMG recordings from patients tested with TMS within 1 week of stroke.
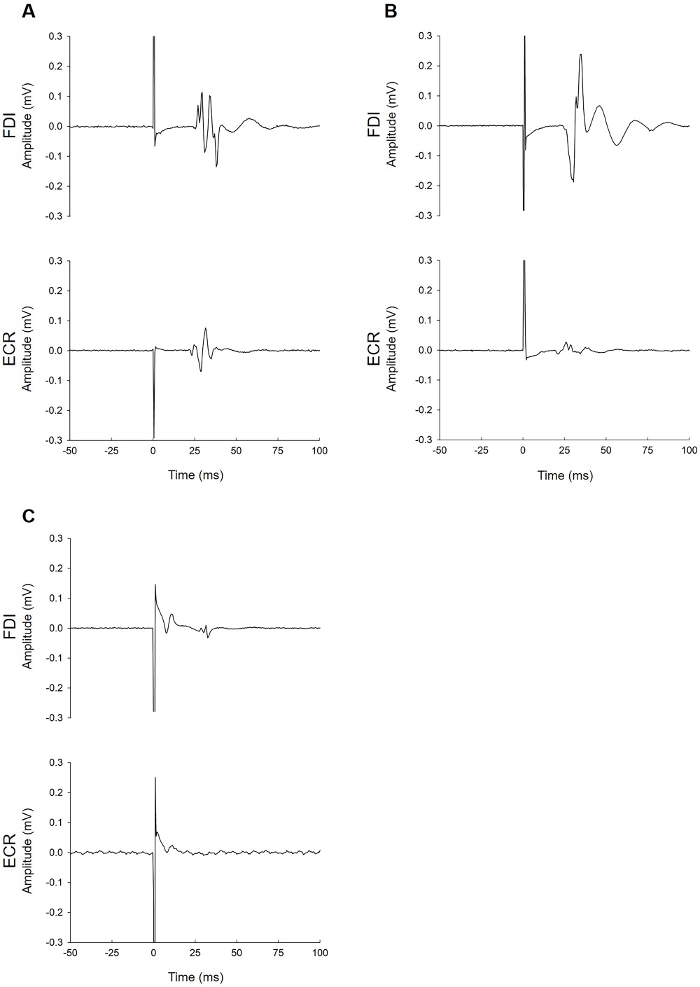
Figure 2: Examples of MEP+ patients. (A) This patient had MEPs in the paretic FDI (top trace) and ECR muscles (bottom trace). The FDI MEP latency (25 ms) was slightly longer than ECR (21 ms), as expected. (B) This patient had MEPs in the FDI and ECR muscles. The ECR MEP amplitude was small (40 µV) but occurred at an appropriate latency. While this patient clearly had a large FDI MEP, they would be considered MEP+ based on the ECR trace alone. (C) This patient had a small MEP in the FDI muscle (40 µV) and no MEP in the ECR muscle. The MEP occurred at an appropriate latency (27.5 ms). This patient can be considered MEP+ because the MEP was observed on at least five traces (see step 3.8.1 in protocol). Please click here to view a larger version of this figure.
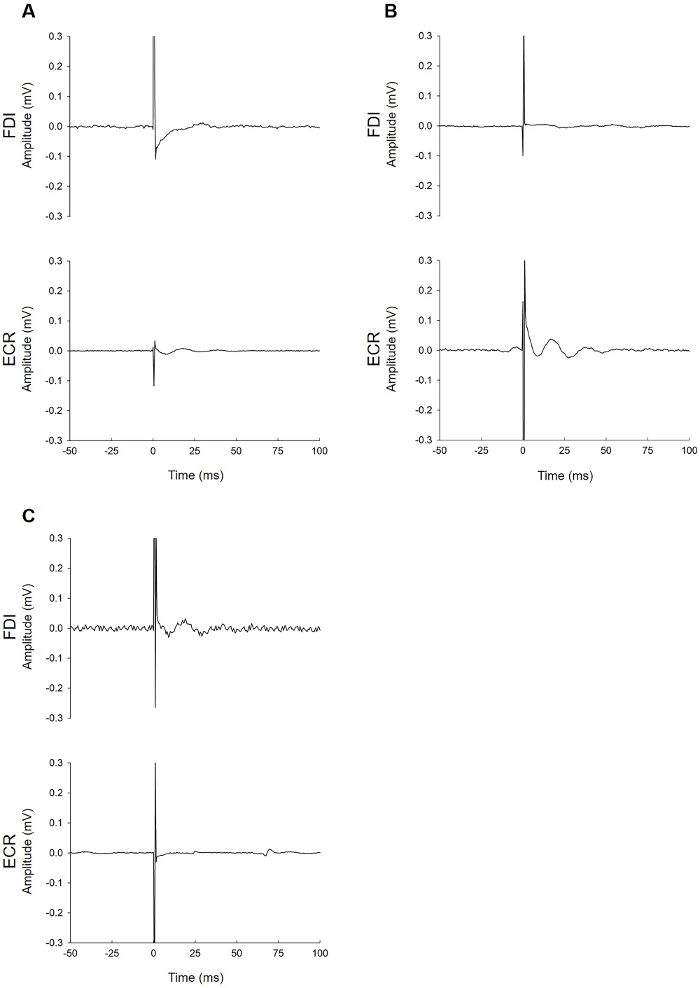
Figure 3: Examples of MEP-patients. These patients failed to demonstrate MEPs at 100% MSO while at rest and attempting active bilateral facilitation to increase the likelihood of eliciting a MEP. The EMG traces do not show muscle activity during facilitation due to severe paresis. (A) This patient had no MEP of any amplitude in either muscle despite all efforts to elicit one. (B) This patient had no MEP in the FDI muscle (top trace). The bottom trace (ECR) contains an elongated tail of the stimulus artifact. When this is present during the latency window for either muscle, identification of a MEP can be difficult. See Figure 4 for advice on troubleshooting EMG noise issues. If the problem cannot be solved, the result of the FDI trace is used, which in this case is MEP-. (C) The fluctuation seen in the ECR muscle EMG trace is not a MEP. This is a motor unit firing sporadically. These can be identified due to their uniform shape and appearance at latencies that do not correspond with the expected latency for ECR. Please click here to view a larger version of this figure.
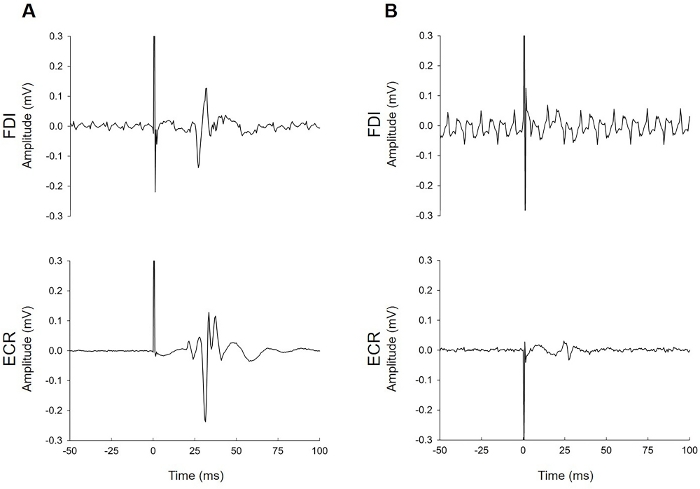
Figure 4: Examples of EMG traces contaminated by electrical noise. (A) This patient had MEPs in both muscles that are clearly identifiable despite the electrical noise in the FDI trace. (B) This patient had MEPs only in the ECR. Noisy signals can be a common problem during EMG recording. The researcher needs to consider whether the noise is environmental (due to issues with electrical noise in the room, or in the EMG setup) or biological (underlying muscle activity from the patient). Troubleshooting suggestions include but are not limited to checking whether skin preparation was adequate, the electrode has lost contact with the skin (this is particularly common with FDI if a patient has perspiration on their hands), issues with the grounding strap or electrode, cables are firmly attached to the patient and the EMG unit, anyone is touching the patient or the TMS trolley during the test, unplugging the bed from its electrical power supply, adjusting lighting (turning off fluorescent lighting), and adjusting the patient position so that they are able to relax with their ULs fully supported on pillows. In both of these traces, the background noise was only present in one muscle. This suggests that noise issues were specific to the setup for that muscle (e.g., a loose cable, poor electrode conduction due to a lack of contact with the skin, or a faulty electrode). Noise that is present in the traces for both muscles indicates issues with the grounding electrode or strap or electrical noise in the environment. Please click here to view a larger version of this figure.
