Six animals were subjected to the surgery protocol described above. The control group as shown in the Figure 4 consisted of six rats. The brain slices shown in the Figure 4 were derived from one rat per group.
The MRI scanning showed that the infarction was located in the basis of the pons (Figure 4A). Since the probe was injected 2 mm to the left of the midline, the infarction was located laterally. This infarction mimics anterolateral pontine infarctions in patients (Figure 4A). Because an insulated sheath was used, there was no infarction beyond the tip of the probe including the cortex, cerebellum, and midbrain (Figure 4A). DWI images also revealed the acute pontine infarction (Figure 4A).
TTC staining was used to confirm the infarction 24 h post-surgery (Figure 4A). Compared to the control group, the infarction volume was significantly higher (Figure 4B).
Behavioral scores were measured before and after surgery. The scores for the control and infract model groups before and after surgery are presented in Table 1. Due to the lack of a specific behavioral test designed for pontine infarction, the Longa score, Berderson score, and balance beam test were used to assess the neurological deficits. Additionally, the adhesive removal somatosensory test to assess the sensorimotor function as well as limb-placement test to assess the proprioception.
Compared to the control group, the rats with pontine infarction circled to the left (Figure 4A). There were significant differences in Longa score (2.67 ± 0.52 vs. 0, p < 0.05, Figure 4C), Berderson score (2.67 ± 0.52 vs. 0, p < 0.05, Figure 4D), limb placement test (4.67 ± 0.52 vs. 0, p < 0.05, Figure 4E), beam balance test score (118.33 ± 2.66 vs. 10.17 ± 1.47, p < 0.05, Figure 4F), and adhesive removal somatosensory test score (2.33 ± 0.52 vs. 12.0 ± 0, p < 0.05, Figure 4G) between rats with pontine infarction and control group rats.

Figure 1: Infarction establishment. (A) A hole made in the skull. (B) The sheath is moved to the hole. (C) Injection of the sheath. (D) Injection of the probe. (E) The anode (red arrow) is connected. (F) The probe is removed. (G) Hole (red arrow) left in the brain surface. Please click here to view this video. (Right-click to download.)
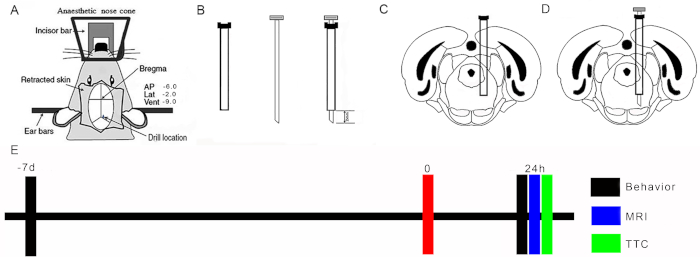
Figure 2: Location of probe. (A) Schematic diagram of stereotaxic locations: arrows point to retraction of skin flaps, site of Bregma, and positioning of drill. (B) Schematic diagram of the sheath and probe. (C) Location of tip of sheath placed in the pons. (D) Location of tip of the probe placed in the pons. (E) Experimental design. Please click here to view this video. (Right-click to download.)
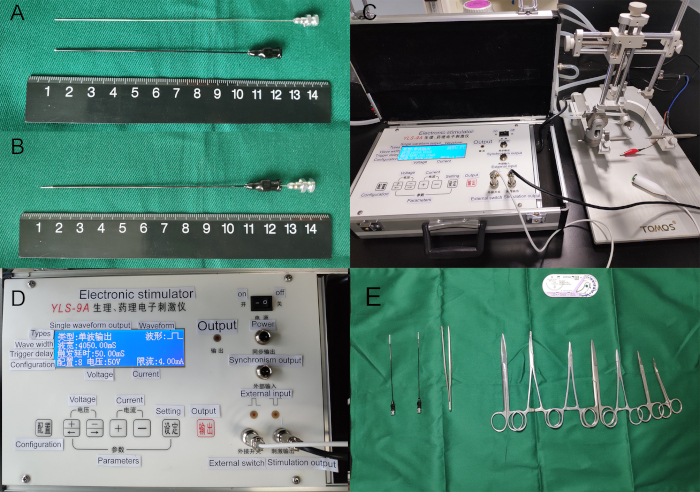
Figure 3: Lesion-producing device. (A) Separate of sheath and probe. (B) The probe in the sheath. (C) The blue electrode was anode which was connected to the caudal probe; the red electrode was cathode. (D) Electrical stimulator. (E) Surgical instruments. Please click here to view this video. (Right-click to download.)
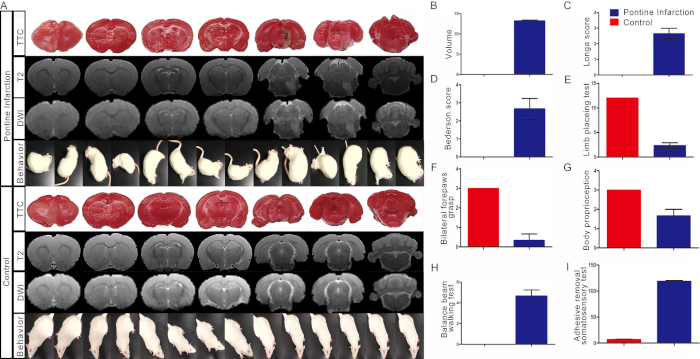
Figure 4: Representative results. (A) The infarction was assessed by MRI scanning with T2 and DWI sequence in vivo and was confirmed by TTC staining in vitro 24 h after surgery. Acute pontine infarction located in the right anterolateral pons (dotted line). Behavioral test showed that the rat circled to the contralateral side of lesion. (B) The volume of infarction. (C) Long score. (D) Bederson score. (E) Limb placing test. (F) Balance beam walking test. (G) Adhesive removal somatosensory test. Bars represent mean ± SD (p < 0.05 vs. control group). Please click here to view this video. (Right-click to download.)
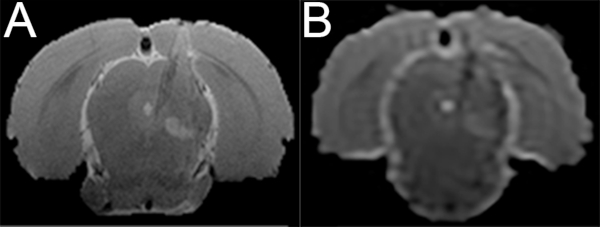
Figure S1: Lacunar infarction in the pons. The length of the probe tip is shortening. MRI scanning shows a lacunar infarction in the right pons. (A) T2 image. (B) DWI image. Please click here to view this video. (Right-click to download.)
| Rat NO | Longa score | Berderson score | Balance beam test | Adhesive-removal somatosensory test | Limb-placement test | |||||
| Pre | Post-surgery | Pre | Post-surgery | Pre | Post-surgery | Pre | Post-surgery | Pre | Post-surgery | |
| Pontine infarction 1 | 0 | 3 | 0 | 2 | 0 | 5 | 6 | 120 | 12 | 2 |
| Pontine infarction 2 | 0 | 2 | 0 | 3 | 0 | 4 | 8 | 120 | 12 | 3 |
| Pontine infarction 3 | 0 | 3 | 0 | 3 | 0 | 5 | 8 | 116 | 12 | 2 |
| Pontine infarction 4 | 0 | 3 | 0 | 3 | 0 | 4 | 6 | 120 | 12 | 2 |
| Pontine infarction 5 | 0 | 3 | 0 | 2 | 0 | 5 | 7 | 114 | 12 | 2 |
| Pontine infarction 6 | 0 | 2 | 0 | 3 | 0 | 5 | 7 | 120 | 12 | 3 |
| Control 1 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 11 | 12 | 12 |
| Control 2 | 0 | 0 | 0 | 0 | 0 | 0 | 8 | 10 | 12 | 12 |
| Control 3 | 0 | 0 | 0 | 0 | 0 | 0 | 10 | 8 | 12 | 12 |
| Control 4 | 0 | 0 | 0 | 0 | 0 | 0 | 7 | 11 | 12 | 12 |
| Control 5 | 0 | 0 | 0 | 0 | 0 | 0 | 8 | 9 | 12 | 12 |
| Control 6 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 12 | 12 | 12 |
Table 1: Behavioral scores.
