A schematic illustration of the cytokine stimulations used for polarization of monocyte-derived cells to M0 (M2-like cells), M1 (fully polarized M1 cells) and M2 (fully polarized M2 cells) is presented in Figure 1A, while representative images of M0, M1 and M2 cell cultures as well as M1 cultures at day 0, 3 and 7, are shown in Figure 1B. Uninfected M0 cells were used to demonstrate the basic gating strategy (Figure 2A). Initially, the myeloid cells (~85%) were gated according to their forward scatter (FSC) and side scatter (SSC) properties including the larger cells with high granularity and excluding the small-sized debris with a low SSC and FSC that are found at the bottom left corner of the dot plot. In the second plot, doublets (i.e., cell clumps) were defined as having an increased area but similar height compared to single cells and were excluded from further analysis. Therefore, only cells proportionate between FSC-Area and FSC-Height (single cells) were included inside the slanted shape gate. Next, the Zombie-UV viability dye that stains the cytoplasmic proteins inside the dead cells, was used to exclude the dead cells from subsequent analysis. As expected, viable uninfected M0 cells were negative for Mtb-GFP expression visualized in the FITC-channel.
Next, we applied the same gating strategy to uninfected as well as Mtb-infected M1 and M2 macrophages at 4 hours post-infection (Figure 2B,C). Two sub-populations were detected in the FCS/SSC gate of uninfected M1 polarized macrophages; one population with a smaller size (FCS) and higher granularity (SSC) and the other population with a larger size and lower granularity (Figure 2B), while the main gate of uninfected M2 cells appeared more homogenous (Figure 2C). Both M1 and M2 monocyte-derived cells displayed a vertical shift to higher granularity and reduced cell size upon Mtb infection, which may reflect an increased complexity inside the cells caused by uptake of intracellular Mtb bacteria (Figure 2B,C). Furthermore, the viability stain revealed an enhanced cell death (17-22%) among the Mtb-infected M1 and M2 cells at a MOI of 5, compared to uninfected M0 cells (99%) (Figure 2A-C) or uninfected M1 and M2 cells (data not shown). Representative data showed that Mtb-GFP expression (i.e., Mtb infectivity) was substantially higher in M2 (77% GFP-positive cells) compared to M1 (19% GFP-positive cells) cells after 4 hours of infection (Figure 2B,C). After 24 hours of infection, Mtb-GFP expression was 43% and 85% in M1 and M2 cells respectively, suggesting that M1 cells had a relatively higher increase in GFP-expression from 4–24 hour after Mtb infection compared to M2 cells, 126% versus 10.4% increase in GFP-expression in M1 and M2 cells from 4–24 hours, respectively.
To characterize the efficacy of M1/M2 polarization in uninfected monocyte-derived cells, dot plots were used to identify M1 cells that were double-positive for CD64 and CD86 (CD64+CD86+) and M2 cells that were double-positive for CD163 and CD200R (CD163+CD200R+; Figure 3A,B). The selection of M1/M2 markers was primarily made based on the results from our previous work25 but also from other studies26,27,28,29. The quadrants for the stained cells, were set using corresponding gates for unstained M1/M2 cells (Figure 3A). None of these markers is exclusively expressed by M1 or M2 cells, but the proportion of positive cells as well as the intensity of the surface expression is different. This was particularly evident from the M1 stain where around 95% of M1 cells and 79% of M2 cells were CD64+CD86+, but the staining intensity was substantially higher in the M1 subset (Figure 3A). Whereas 27% of M1 cells were positive for the M2-marker CD200R, only 1% were positive for CD163, providing 0.5% CD163+CD200R+ M1 cells compared to 63% CD163+CD200R+ M2 cells (Figure 3A). After 4 hours of Mtb infection, an increase in the frequency of CD200R+ cells was observed in Mtb-GFP-positive M1 polarized cells (16%), while CD163-expression was reduced in M2 cells (Figure 3B). The heat-map demonstrates a high intensity of GFP-expression in CD163+CD200R+ M2 cells, but also in the CD64+CD86+ M2 subset as compared to the corresponding M1 cells subsets (Figure 3B). Overall, the shift in expression of the respective M1 and M2 markers is also visualized in the histograms in Figure 3C. Furthermore, Mtb-GFP bacteria were also visualized in CD64+ M1 cells and in CD163+ M2 cells by confocal microscopy, which supported an enhanced intracellular uptake and/or growth of Mtb inside M2 compared to M1 cells (Figure 3D).
To verify the results of the manual gating, we applied dimensionality reduction using Uniform Manifold Approximation and Projection (UMAP). UMAP analysis showed that Mtb infection for 4 hours was not sufficient to affect the polarization of macrophages, in contrast to 24 hours of infection, which resulted in clearly separated clusters of M1 and M2 uninfected and infected cells (Figure 4A). Uninfected M1 macrophages displayed higher expression of CD64, CD86, TLR2, HLA-DR and CCR7 compared to M2 macrophages, while uninfected M2 cells exhibited a strong up-regulation of the M2 phenotype markers CD163, CD200R, CD206 and CD80 (Figure 4B,C). In agreement to the manual gating, Mtb infection after 24 hours caused a clear downregulation of CD163, CD200R and CD206 on M2 cells and upregulation of CD86 and HLA-DR on M1 cells (Figure 4B,C), which suggests that Mtb can modulate macrophage polarization. Subsequent phenograph analysis (Figure 4D-F) identified 24 different clusters of different sizes that were uniquely distributed among the M1 and M2 uninfected and Mtb-infected cells as illustrated in the UMAP graphs (Figure 4D), pie charts (Figure 4E) and heat-maps (Figure 4F). Altogether, these results show promising efficiency of this protocol to generate phenotypically and functionally diverse M1 and M2 polarized cells in vitro that are further modulated by Mtb infection.
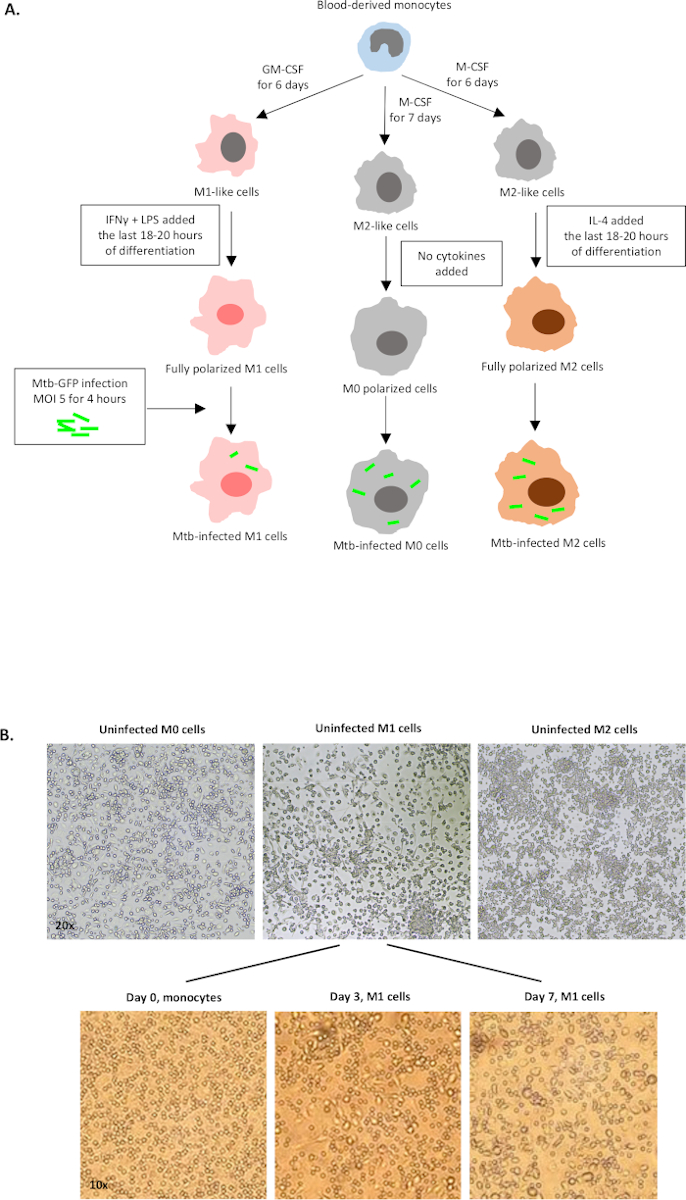
Figure 1: Schematic illustration of in vitro differentiation and polarization of human myeloid-derived cells. (A) M0 (M2-like), M1 (classically activated) and M2 (alternatively activated) cells are depicted. Monocytes obtained from healthy blood donors were polarized with different cytokines as described in the protocol and infected with the GFP-labeled Mtb strain, H37Rv, for 4 hours before analysis with 10-color flow cytometry. M1-polarized cells typically contain fewer bacteria compared to M2-polarized cells. (B) Microscopic images of fully polarized, uninfected M0, M1 and M2 cells in the 6-well plates at day 7, and representative images of M1 cell differentiation from monocytes at day 0, 3 and 7. Magnification is 20x (upper panel) and 10x (lower panel). Note that the M1 cells are more elongated and stretched compared to the more rounded M0 and M2 cells (upper panel). Please click here to view a larger version of this figure.
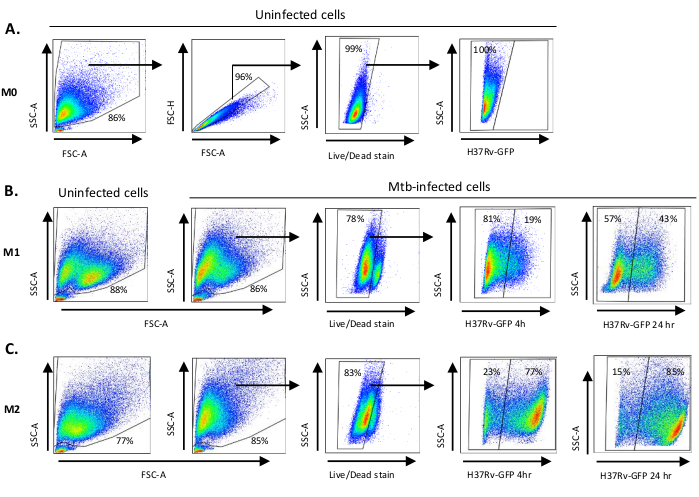
Figure 2: Gating strategy of differentially polarized myeloid-derived cells. Representative dot plots showing (A) Forward scatter (FSC) and side scatter (SSC) properties of uninfected M0 macrophages. The FSC-A/FSC-H plot shows manual gating of single cells proportionate for area and height. The live cell gate excluded cells that were positive for Zombie-UV (viability dye). Intracellular Mtb was detected by GFP-expression in live cells observed in the FITC channel. (B) Gating of M1 and (C) M2 macrophages showing FCS/SSC dot plots of both in uninfected cells and Mtb-infected cells 4 h and 24 h post-infection. Please click here to view a larger version of this figure.
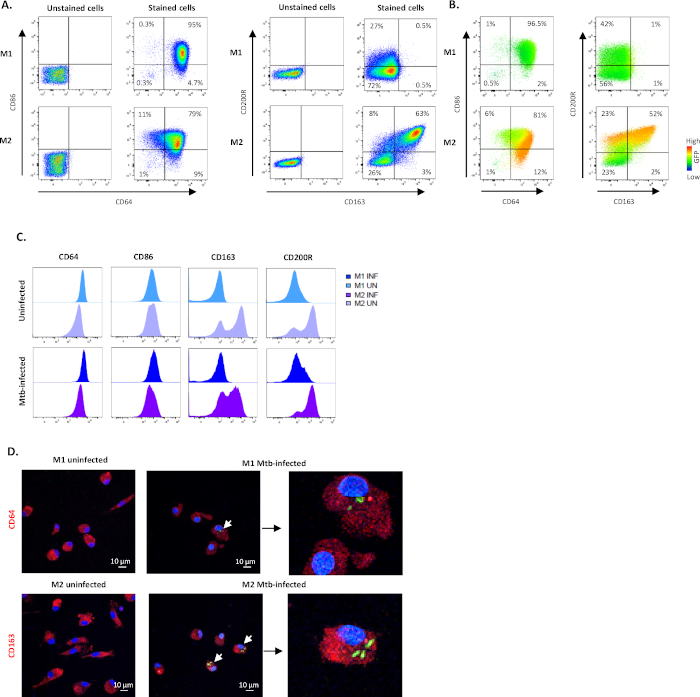
Figure 3: Efficacy of the in vitro M1/M2 polarization protocol. Representative dot plots and quadrant gating showing subset frequencies of M1- and M2-polarized cells using CD64 and CD86 (M1) or CD163 and CD200R (M2) in (A) unstained and stained uninfected cells and (B) Mtb-infected stained cells 4 h post-infection. The dot plots in (B) illustrates fluorescence intensity of GFP-expression (heat map) in M1- and M2-polarized macrophages obtained from different sub-gates. (C) Geometric mean of fluorescence intensity (MFI) is shown in histograms from one representative donor after 4 h of Mtb infection. The MFI values in uninfected M1 (light blue) and M2 cells (light purple) are presented in the upper panel and Mtb-infected M1 (deep blue) and M2 cells (deep purple) are presented in the lower panel. (D) Representative confocal images of uninfected and Mtb-infected M1- and M2-polarized cells is shown. M1 and M2 cells were stained for CD64 and CD163 expression, respectively, using immunofluorescence. Positive surface staining is shown in red and GFP-expressing intracellular bacteria is shown in green. DAPI-stained nuclei are shown in blue color. Scale – 10 µm. The magnification of images to the right is 350x. Please click here to view a larger version of this figure.
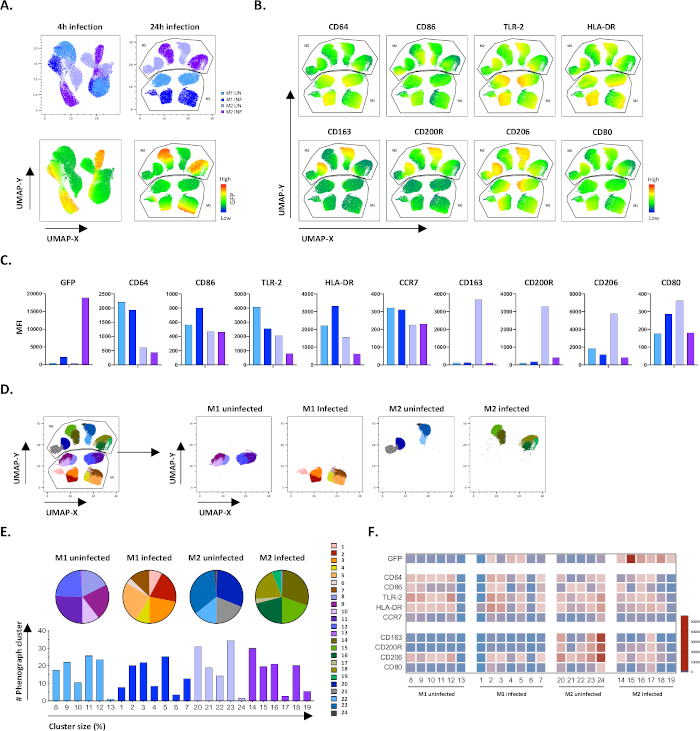
Figure 4: Dimensionality reduction with Uniform Manifold Approximation and Projection (UMAP) and phenograph analysis of uninfected and Mtb-infected M1 and M2 cells. (A) UMAP, created by concatenating 11000 live cells from uninfected and Mtb-infected M1 and M2 cell cultures from two representative blood donors, 4 h (left graphs) or 24 h (right graphs) post-infection. The heatmap for GFP-expression (lower panel) indicates uninfected and Mtb-infected cells. (B-C) MFI of markers expressed in uninfected and Mtb-infected M1 and M2 cells 24 h post-infection, shown as (B) heatmap or (C) bar plots. (D-F) Phenograph analysis identified 24 clusters that are differentially distributed among the uninfected and Mtb-infected M1 and M2 cultures. Clusters 8–13 are unique in uninfected M1 cells, clusters 1–7 are unique in Mtb-infected M1 cells, clusters 20–24 are unique in uninfected M2 cells and clusters 14–19 are unique in Mtb-infected M2 cells. The MFI of each marker in each phenograph cluster is shown in (F). The data is presented as uninfected M1 (light blue) and M2 cells (light purple) and Mtb-infected M1 (deep blue) and M2 cells (deep purple). Please click here to view a larger version of this figure.
Table 1: List of antibodies used for flow cytometry.
| Laser | Filter | Fluorochrome | Phenotype | Function | Clone | Catalog no. | Company |
| 639 | 670/30 | AF647 | TLR2 | Pathogen recognition receptor | TL2.1 | 309714 | BioLegend |
| 639 | 780/60 | APC-Cy7 | CD206 | Mannose receptor | 15-2 | 321120 | BioLegend |
| 405 | 610/20 | BV605 | CD163 | Scavenger receptor | GHI/61 | 333616 | BioLegend |
| 405 | 670/30 | BV650 | CD80 | Co-stimulatory molecule | 2D10 | 305227 | BioLegend |
| 405 | 710/50 | BV711 | CCR7 | Chemokine receptor | G043H7 | 353228 | BioLegend |
| 405 | 780/60 | BV785 | CD86 | Co-stimulatory molecule | IT2.2 | 305442 | BioLegend |
| 488 | 530/30 | GFP | Mtb | Intracellular bacteria | |||
| 561 | 586/15 | PE | CD200R | Inhibitory receptor | OX-108 | 329306 | BioLegend |
| 561 | 620/14 | PE/DAZZLE 594 | CD64 | Fc gamma receptor-I of IgG | 10.1 | 305032 | BioLegend |
| 561 | 661/20 | PE-Cy5 (PC5) | HLA-DR | MHC class II molecule | L243 | 307608 | BioLegend |
| 355 | 450/50 | BUV395 | Viability Dye | Live/dead cell marker | Zombie UV | 423108 | Invitrogen |
