In this protocol, we describe a step-by-step method for inducing a model of experimental autoimmune uveitis (EAU) by immunizing mice with a uveitogenic retinal peptide derived from IRBP. The assessment of disease employing widely used and readily accessible approaches are covered although these are not exclusive and may be added to, or partially replaced, by other imaging techniques. The first signs of EAU in C57BL/6J mice can be detected two weeks post-immunization and peak disease reached within three weeks as illustrated in Figure 1. Fundoscopic changes are classified during disease progression as inflammatory changes, which include retinal tissue, vascular and optic disc inflammation, and retinal structural damage (Figure 2) in addition to histological changes based on infiltrating immune cells and structural damage. These clinical and histopathological changes can be detected for up to 85 days post immunization, and graded and scored for evaluation proposes to study disease progression. In order to avoid unintentional bias in the qualitative visual scoring, the images should be evaluated by more than one expert and scorers require to be blinded to the treatment groups.
We show here how the clinical and histological scoring systems (Table 1 and Table 2) guide scientists to quantify EAU severity, to validate the efficacy of treatments and to explore the mechanism of drug action. Vascular leakage is also a pathological feature of the model and in human uveitis. We are showing examples of vascular leakage of fluorescein (Figure 3) as another method for assessing disease in this model.
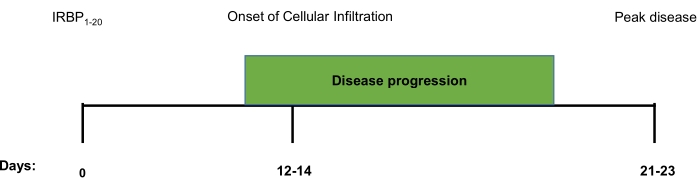
Figure 1. Schematic timeline of clinical and histological disease progression in IRBP1-20 induced EAU. A timeline marking the onset of infiltration and progression of IRBP1-20 induced EAU towards peak disease. From immunisation, the first signs of clinical disease, as detected by fundoscopic imaging and histopathological analysis, falls between days 12-14. The disease will then continue to progress, according to these parameters, until a peak is reached around day 21-23. Please click here to view a larger version of this figure.
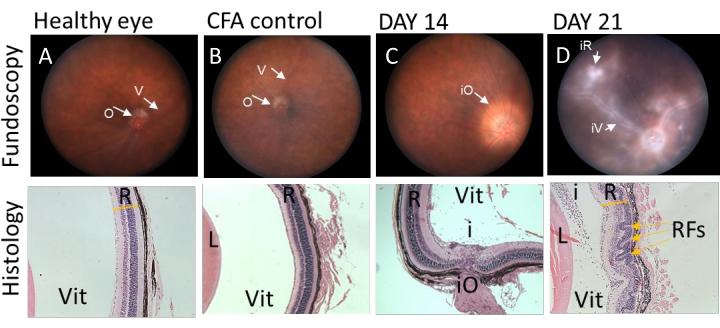
Figure 2. Representative fundoscopic images correlating with histological sections at different stages of IRBP1-20 induced EAU disease in C57BL/6J mice. Clinical fundoscopic and corresponding tissue images of C57BL/6J from the same animal immunised with IRBP1-20 peptide. (A and B) fundoscopic images and histological sections of eye obtained from healthy and CFA injected mice. Retina has no sign of inflammation and corresponding histology sections show preserved retinal layers. (C) Fundoscopic image of eye obtained from C57BL/6J mouse 14 days post immunization demonstrate classic signs of EAU, presenting with severe optic disc swelling in the early stage of disease, corresponding histology shows infiltrating immune cells into vitreous space. (D) Fundoscopic images of eye obtained from C57BL/6J mouse 21 days post immunization shows signs of vessel cuffing and infiltrating immune populations. Histology data demonstrates severe structural changes by retinal folding (yellow arrows). V= vessel, O= optic disk, R=retina, L=lens, Vit=vitreous, iO= inflamed optic disk, iV= inflamed vessel, iR= inflamed retina, i= infiltrating cells in vitreous, RFs=retinal folds. Please click here to view a larger version of this figure.
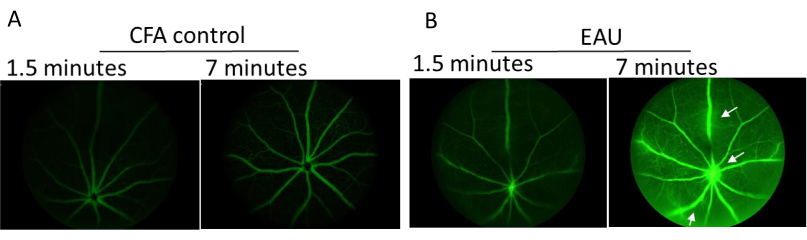
Figure 3. Representative images of fluorescent angiography taken using Micron III imaging system at peak disease. C57BL/6J mice were injected subcutaneously with 2% fluorescein and images taken at various timepoints after circulation of the tracer. (A) CFA only control mouse taken at 1.5- and 7-minutes post fluorescein administration. (B) Representative images of IRBP1-20 immunized mice taken 1.5 and 7 minutes, respectively, after receiving fluorescein. White arrow indicates vessel leakage. Please click here to view a larger version of this figure.
| Score | Optic Disc | Retinal Vessels | Retinal Tissue Infiltrate | Structural Damage | ||||
| 1 | Minimal Inflammation | 1-4 mild cuffings | 1-4 small lesions or 1 linear lesion | Retinal lesions or retinal atrophy involving ¼ to ¾ retina area | ||||
| 2 | Mild inflammation | >4 mild cuffings or 1-3 moderate cuffing | 5-10 small lesions or 2-3 linear lesions | Pan retinal atrophy with multiple small lesions (scars) or <3 linear lesions (scars) | ||||
| 3 | Moderate inflammation | >3 moderate cuffings | >10 small lesions or >3 linear lesions | Pan retinal atrophy with >3 linear lesions or confluent lesions (scars) | ||||
| 4 | Severe inflammation | >1 severe cuffing | Linear lesion confluent | Retinal detachment with folding | ||||
| 5 | * Not visible (white out or extreme detachment) | * Not visible (white out or extreme detachment) | * Not visible (white out or extreme detachment) | * Not visible (white out or extreme detachment) | ||||
Table 1. Conventional clinical scoring scale for evaluating EAU clinical disease severity. Table showing criteria used to evaluate the extent of disease severity in mice immunised with IRBP1-20. Scores were allocated according to the hallmarks outlined above being visible on the fundus images, each eye was given a total score out of twenty. * Due to the obscuration of infiltrate and retinal detachment inside the posterior chamber cannot be assessed. Table adapted with permission from Xu H., et al., 20088.
| Grade | Criteria |
| 0 | No change |
| 0.5 (trace) | Mild inflammatory cell infiltration. No tissue damage |
| 1 | Infiltration; retinal folds and focal retinal detachments; few small granulomas in choroid and retina, perivasculitis |
| 2 | Moderate infiltration; retinal folds, detachments and focal photoreceptor cell damage; small to medium sized granulomas, perivasculitis and vasculitis |
| 3 | Medium to heavy infiltration; extensive retinal folding with detachments, moderate photoreceptor cell damage; medium sized granulomatous lesions; subretinal neovascularization |
Table 2. Histologically scoring EAU
Table showing criteria used to evaluate the severity of EAU based on histopathological features of disease. Scores were allocated according to the hallmarks outlined above on H&E staining, each eye was given a total score out of four. Table adapted with permission from Agarwal et al. 201311.
