Women have an increased risk of aSAH compared to men. Despite this, male rodents are primarily used in experiments due to possible bias from heterogeneity of estrus cycle in females. The representative results presented here are from a recent publication comparing female and male rats, confirming that the model produces similar results in female animals compared to male21. The study included 34 female Sprague-Dawley rats (18 SAHs and 16 shams). Shams did not have the spinal needle descended to the optic chiasm or blood injected. All other procedures were performed on Shams identical to SAHs. All the physiological parameters between groups were comparable. Lastly, a meta-analysis of data from previous experiments on the male rats was done and compared with the results of the present study21.
The rotating pole test is a test of gross sensorimotor function. The animal is placed on one end of a 150 cm by 45 mm pole, which can rotate up to 10 rpm. The goal is to reach the far end of the pole where a cage is placed. SAH rats did significantly worse on day 1 and 2, compared to sham animals on the rotating pole (Figure 1).
Following SAH, both the ET-1 and 5-HT receptor family are upregulated in the cerebral arteries resulting in an increased contraction when stimulated and thereby contributing to CVS22,23.The basilar artery (BA) and middle cerebral arteries (MCA) were removed following decapitation and used for myograph experiments. Both endothelin 1 (ET-1), an agonist for the ET-1 receptor family and 5-carboxamidotryptamine (5-CT), an agonist for the 5-HT-receptor family produced significantly increased vascular contraction in SAH compared to sham (Figure 2). Sensitivity can be observed by the lower concentrations needed to elicit contraction following SAH in both sexes.
Increased water content (edema) following SAH is a measure of reduced functional outcome in humans24. Significantly increased cerebral edema was found in SAH compared to sham on day 2. There was also a tendency toward increased edema in the hippocampus, but this was not statistically significant (p = 0.0508)21.
When comparing the above-mentioned data to historical male data, the results are comparable. The metadata shows increased contractility in male SAHs following addition of ET-1 or 5-CT (Figure 2). Furthermore, the SAH rats performed significantly worse compared to shams when doing the rotating pole test. The result indicated a decreased sensorimotor function (Figure 1).
Figure 5A shows the distribution of the autologous, injected blood following saline perfusion 30 min after induction of the SAH. The figure shows that the blood has been distributed in the subarachnoid space following pre-chiasmatic injection.
Figure 5B and Figure 5C shows the distribution of intrathecally injected dyes, followed by whole body saline perfusion for 30 min after the injection. Figure 5B shows the distribution of 25 µL of 20 mM Evans Blue (water soluble) and Figure 5C shows the distribution of 25 µL of 10 mM Oil Red O (water insoluble). Both dyes were found to be distributed in the subarachnoid space following the injection into the cisterna magna, confirming that this is a feasible model of intrathecal injection of both water soluble and insoluble compounds. Worth noticing is the formation of deposits around the arteries for the water insoluble compound.
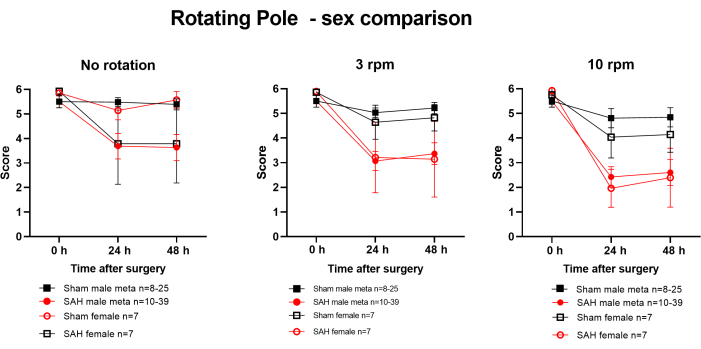
Figure 1: Analysis of sensory-motor cognition in the first 2 days after SAH in male and female rats. Rotating pole test was performed on day 1 and day 2 after SAH. Rats of both genders had significant deficits compared to sham-operated rats of the same gender. Statistical differences in behavior between groups were tested by 2-way ANOVA on day 0, day 1, and day 2. Female no rotation and 3 rpm: p < 0.05. Female 10 rpm and all male data: p < 0.01. Values are means ± SEM. Republished with permission from Spray, S. et al.21. Please click here to view a larger version of this figure.
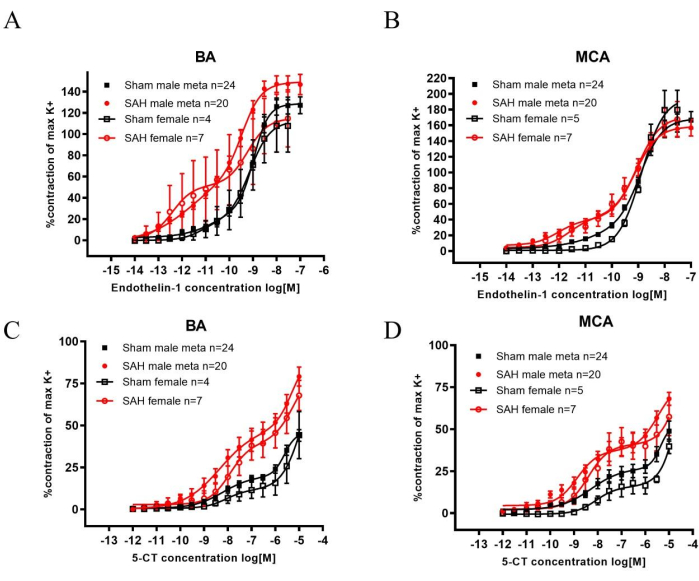
Figure 2: Analysis of increased sensitivity to ET-1 and 5-CT induced contractions in the basilar artery (BA) and middle cerebral artery (MCA) 2 days after SAH in male and female rats. (A,B) 60 mM K+-evoked (K+max) contractile responses were used as reference values for normalization of agonist-induced responses. The sensitivity to ET-1 was significantly increased 2 days after SAH compared to sham-operated rats of the same gender in both the BA and MCA. (C,D) The sensitivity to 5-CT was significantly increased 2 days after SAH compared to sham-operated rats of the same gender in both the BA and MCA. The concentration-response curves were statistically compared with two-way ANOVA. All data: p < 0.001. Values are means ± SEM. Republished with permission from Spray, S. et al.21. Please click here to view a larger version of this figure.
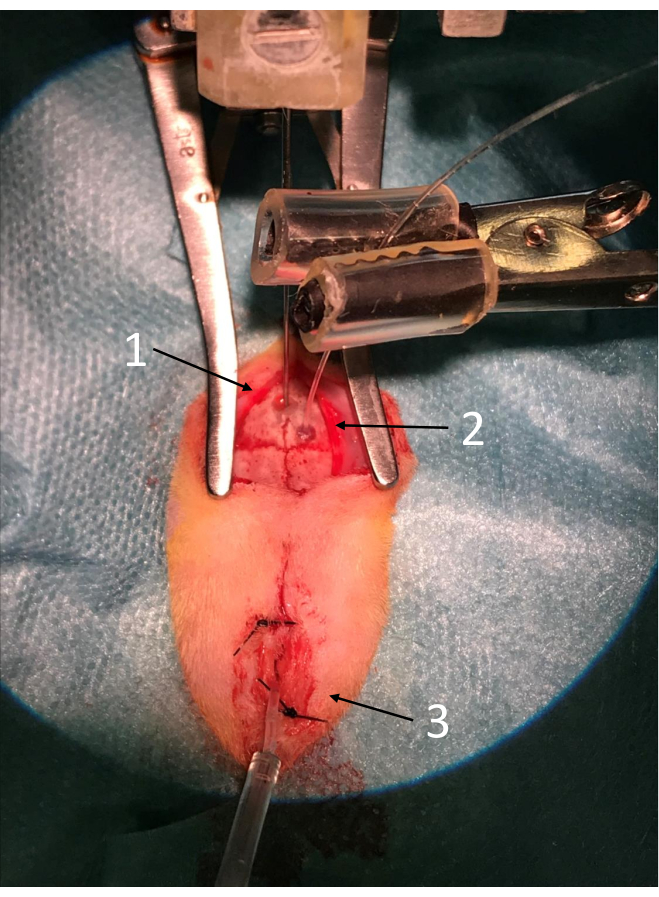
Figure 3: Overview of the setup before induction of SAH. From the top of the picture, note that the 1) injection needle, 2) laser-Doppler probe, and 3) the ICP probe are all in place. Please click here to view a larger version of this figure.
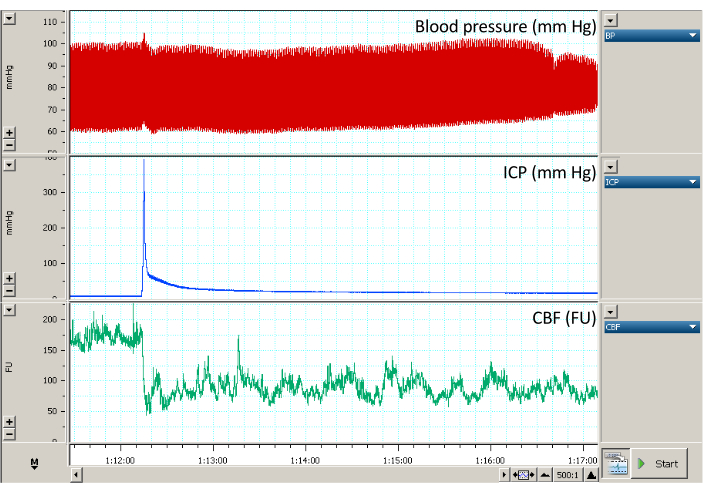
Figure 4: Sample trace following intrathecal injection. The red graph shows the blood pressure in mmHg. The blue graph shows the ICP in mmHg and the green graph shows the CBF in the arbitrary unit FU. The spike in ICP is the result of blood injection. Notice that this results in a drop in the CBF > 50% of baseline for more than 5 min. The ICP rise furthermore results in a small rise in blood pressure which normalizes within seconds. Please click here to view a larger version of this figure.
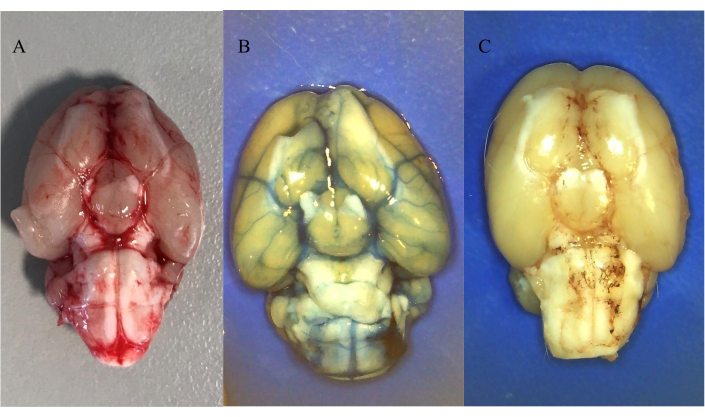
Figure 5: Distribution of intrathecally injected blood and colored dyes. (A) Distribution of autologous blood 30 min after SAH induction. (B) Distribution of 25 µL of 20 mM Evans Blue following intrathecal injection through ICP-catheter. (C) Distribution of 25 µL of 10 mM Oil Red O following intrathecal injection through ICP-catheter. All animals were anesthetized with intraperitoneal ketamine/xylazine mixture followed by saline perfusion. Please click here to view a larger version of this figure.
