Following each resting-state scan, stability is assessed using an independent component analysis (ICA; example script included in Supplementary Files). Figure 6 shows examples of component outputs from resting-state scans. Figure 6a shows a signal component from a scan with high stability. Note that spatially, the component has high regionality. Within the time course below the spatial component, the signal is stable and not predictable, indicative of true brain activity. The power spectrum at the bottom shows predominantly low frequencies. Figure 6b shows a component from the same scan as Figure 6a that represents noise. Note the non-regionality in the spatial component, high-frequency time course, and high frequency peak in the power spectrum. Finally, Figure 6c shows a component from a scan with unstable anesthesia. The time course is variable and irregular. When this occurs, improvements are needed to the anesthetic protocol, commonly to the sealing of the nose cone and the scavenging of waste gases.
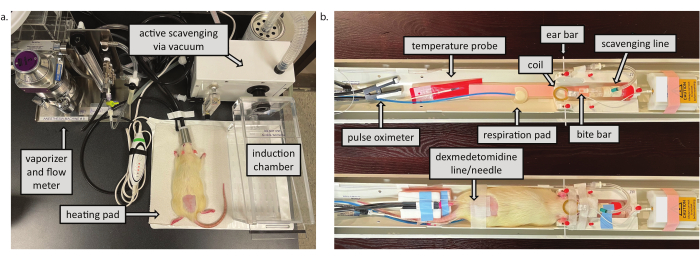
Figure 1: Preparation space and MRI animal cradle. a) Preparation space. The vacuum scavenges waste gases from both the induction chamber and the nose cone at the animal cradle. The heating pad helps to maintain animal temperature during both Phase 1 and recovery. b) MRI animal cradle. The top indicates components of the animal setup in Phase 2. The bottom shows a rat fully set-up and ready for scanning. Please click here to view a larger version of this figure.
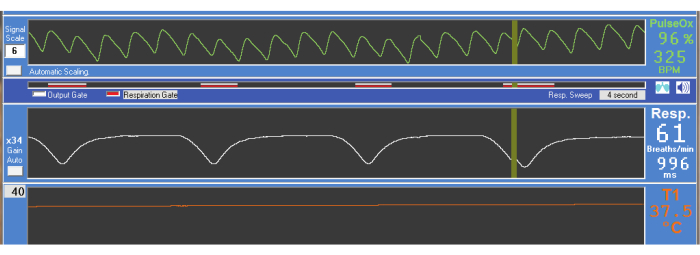
Figure 2: Physiologic scan output. Oxygen saturation (PulseOx, 96%), heart rate (325 BPM [beats per minute]), respiration rate (61 breaths/min), and core body temperature (T1, 37.5 °C) are constantly monitored throughout the scanning session. Please click here to view a larger version of this figure.
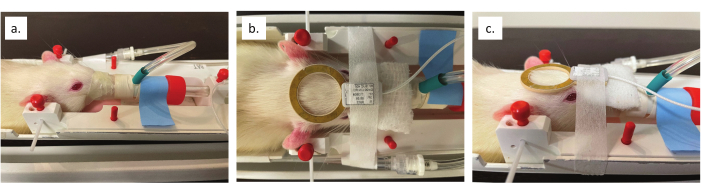
Figure 3: Nose cone and coil placement. (a) Close up view of the nose cone sealed around the animal's nose and lower jaw. (b) Overhead view of the alignment of surface coil to the brain. (c) Side view of coil alignment with the midpoint of the animal's eye. Please click here to view a larger version of this figure.
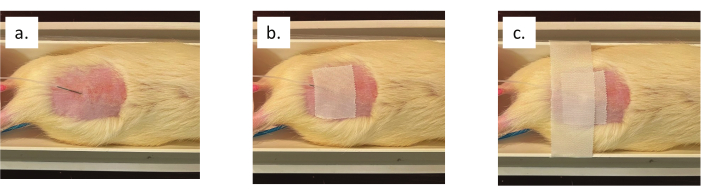
Figure 4: Subcutaneous dexmedetomidine infusion line and needle placement. (a) Needle insertion into the lower lumbar region of the animal's back. (b) Tape securing the needle to the animal's skin. (c) Tape across the animal cradle to prevent movement of the ferromagnetic needle. Please click here to view a larger version of this figure.
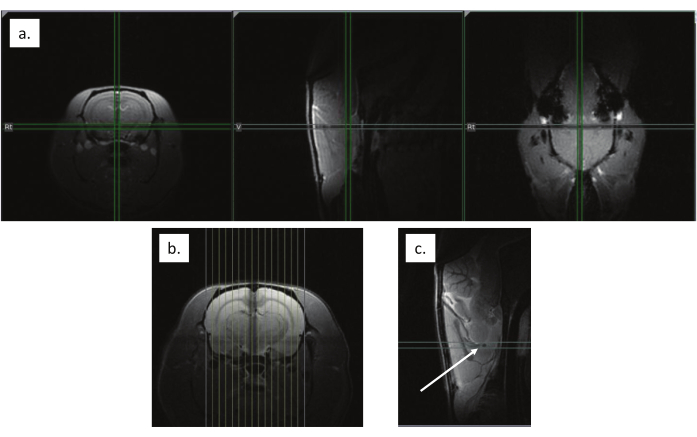
Figure 5: Anatomical scan alignment. (a) Localizer scan to align the animal's brain to the magnet isocenter, noted with crosshairs. (b) Sagittal slices aligned across the brain from left to right. (c) Alignment to the decussation of the anterior commissure, indicated by the white arrow. Please click here to view a larger version of this figure.
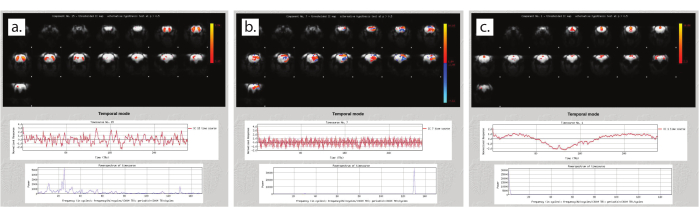
Figure 6: Quality assessment using independent component analysis. (a) Signal component during steady anesthesia. (b) Noise component during steady anesthesia. (c) Unsteady anesthesia. Please click here to view a larger version of this figure.
| Scan | Sequence | Orientation | FOV (mm x mm) | Matrix | Slices | Slice Thickness (mm) | TE (ms) | TR (ms) | Averages | Echo Spacing (ms) | Rare Factor | Repetitions | Scan Time |
| Localizer | FLASH | All planes | 50 | 256 | 1/dir | 1 | 2.5 | 100 | 1 | 1 | 12.8 s | ||
| Localizer | RARE | All planes | 35 | 192 | 1/dir | 0.75 | 28 | 2500 | 1 | 7 | 8 | 1 | 1 min |
| Anat | RARE | Sagittal | 35 | 192 | 15 | 1 | 28 | 2500 | 1 | 7 | 8 | 1 | 1 min |
| Anat | FLASH | Axial | 35 | 192 | 23 | 1 | 5 | 250 | 2 | 1 | 1 min 36 s | ||
| Anat | RARE | Axial | 35 | 192 | 23 | 1 | 28 | 2500 | 4 | 7 | 8 | 1 | 4 min |
| Shim | PRESS | All planes | 16.223 | 2500 | 1 | 1 | 2.5 s | ||||||
| Resting-State | EPI | Axial | 35 | 64 | 15 | 1 | 15 | 1200 | 1 | 300 | 6 min each |
Table 1: Reference table of scan parameters. Parameters for the sequences outlined in the protocol. FLASH = Fast Low Angle Shot, RARE = Rapid Acquisition with Relaxation Enhancement, PRESS = Point RESolved Spectroscopy, EPI = Echo Planar Imaging.
Supplementary Files: Example script for ICA quality assessment. Please click here to download this File.
