The following results were obtained in one healthy subject. RMT for a 200 µV (RMT200) or a 1000 µV (RMT1000) peak-to-peak response were detected by a '4→2→1' tracking rule and logarithmic regression as previously described18. The RMT200 was 52.1% MSO, and the RMT1000 was 59.8% MSO.
All paired-pulse TMS options may be determined in amplitude, parallel threshold-tracking, and serial threshold-tracking modes. Here, only the amplitude and parallel threshold-tracking modes will be summarized. Accordingly, the ISIs, the number of stimuli at each ISI, and the level of stimulus intensity for the conditioning stimuli may be selected from the Menu. Here, we only describe the default options for these.
Figure 1 shows the setup, including stimulation with a figure-of-eight coil, recording with surface electrodes, the computer with installed software, the TMS machine, the noise eliminator to remove 50-60 Hz electrical interference, the isolated linear bipolar constant-current stimulator, the electromyography amplifier, and a data acquisition system.
Figure 2 shows SICI as A-SICI (Figure 2A) and T-SICI parallel (Figure 2B) as described in the protocol section. Figure 3 shows LICI as A-LICI (Figure 3A) and T-LICI parallel (Figure 3B). For A-LICI, after finding the hotspot, the program determines RMT1000 and sets both test and conditioning stimuli to this amplitude. Test-alone stimuli are delivered as every 4th stimulus, and conditioning+test stimuli at intervals of 50, 100, 150, 200, 250, and 300 ms are delivered pseudorandomly. Ten stimuli are delivered at each ISI. Similarly, for T-LICI, 10 paired pulses at the same 6 ISIs as for A-LICI from 50 to 300 ms are delivered, and the thresholds for RMT200 are tracked while conditioning stimulus is set to 120% of the tracked RMT200.
Figure 4 shows SICF as A-SICF (Figure 4A) and T-SICF parallel (Figure 4B). For A-SICF, after finding the hotspot, the program determines RMT50 and RMT1000. Test stimuli are then set to RMT1000 and conditioning stimuli to 90% of RMT50. The range of ISIs is from 1 to 4.9 by 0.3 ms. Test-alone stimuli are delivered as every 4th or 5th stimulus, and the 14 conditioning+test stimuli are delivered in pseudorandom order. As for A-SICF, T-SICF is measured at 14 ISIs from 1 to 4.9 ms, and the threshold is tracked with 10 paired pulses at each ISI.
Figure 5 shows SAI as A-SAI (Figure 5A) and T-SAI parallel (Figure 5B). SAI protocols involve stimulating the somatosensory afferents in the nerve and recording the effects on the MEP excited ~20 ms later. This MEP latency ('N20') is important for the timing of the stimuli. The program asks the user to select the latency from a range (16-23 ms) or to specify it if outside this range. To determine the N20 latency, a conventional somatosensory evoked potential may be performed, or age- and height-corrected laboratory controls may be used.
For the A-SAI, the electrical stimulus intensity for a 1-mV compound muscle action potential is first determined (EMT1000). Then, the hotspot is found for magnetic stimulation, and RMT1000 is determined. The program then combines magnetic and electrical stimuli with ISIs from N20-2 to N20+12 ms. Test-alone stimuli are given as every 4th stimulus, while the conditioning+test stimuli are given in pseudorandom order. For T-SAI similar to A-SAI, EMT1000 is first determined. Then, stimulation switches to the magnetic stimulus, and the hotspot is determined in the usual way. The program then determines RMT200 in a manner similar to the other tracking protocols. Further, the program then runs straight into tracking SAI, with the ISI between electrical stimulus and magnetic test stimulus increased in 1 ms steps from N20-2 to N20+12 ms.
Figure 6 shows LAI as A-LAI (Figure 6A) and T-LAI parallel (Figure 6B). The LAI protocols for recording long-interval afferent inhibition are the same as for SAI, except that because the intervals are much longer (200 to 1000 ms, in 100 ms steps), the N20 interval is disregarded and does not have to be entered.
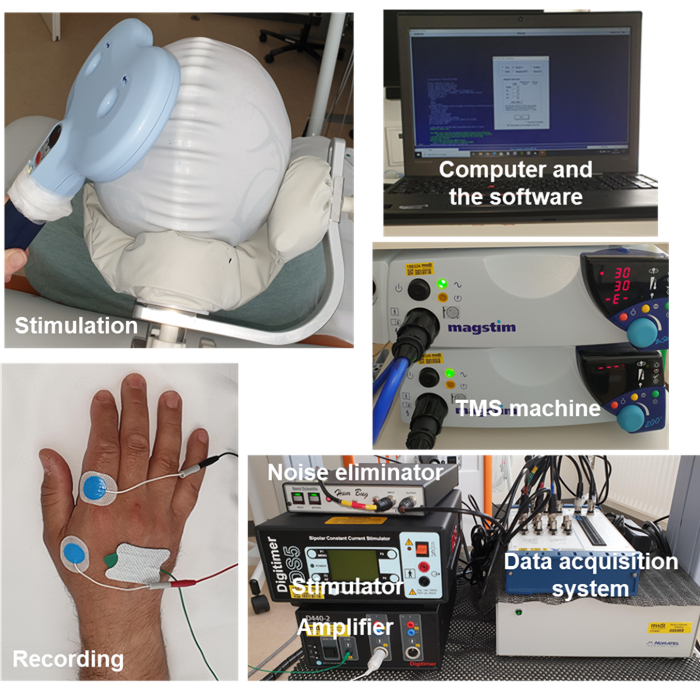
Figure 1: The setup. Setup includes stimulation with a figure-of-eight coil, recording with surface electrodes, the computer with installed software, the TMS machine, the noise eliminator to remove 50-60 Hz electrical interference, the isolated linear bipolar constant-current stimulator, the electromyography amplifier, and a data acquisition system. Abbreviation: TMS = transcranial magnetic stimulation. Please click here to view a larger version of this figure.
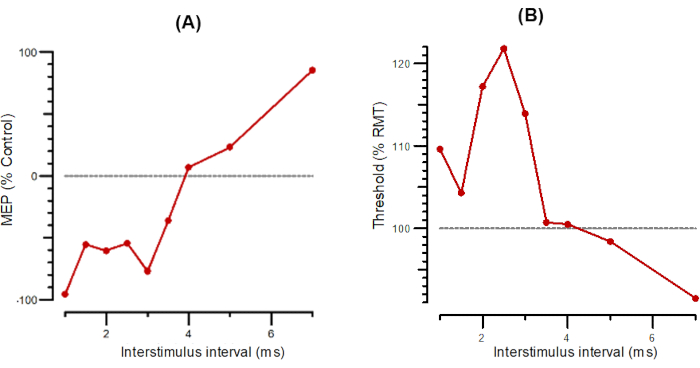
Figure 2: A-SICI and T-SICI plotted as a function of interstimulus intervals from 1 ms to 7 ms. (A) A-SICI plotted as the amplitude of conditioned response as a percentage of control. (B) T-SICI plotted as threshold changes (inhibition as percentage of control). Abbreviations: A-SICI = amplitude of short-interval intracortical inhibition; T-SICI = threshold changes in short-interval intracortical inhibition; MEP = motor-evoked potential; RMT = resting motor threshold. Please click here to view a larger version of this figure.
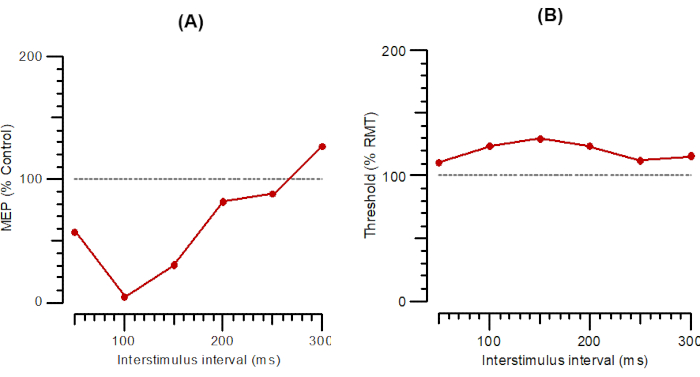
Figure 3: A-LICI and T-LICI plotted as a function of interstimulus intervals from 1 ms to 300 ms. (A) A-LICI plotted as the amplitude of conditioned response as a percentage of control. (B) T-LICI plotted as threshold changes (inhibition as a percentage of control). Abbreviations: A-SICI = amplitude of short-interval intracortical inhibition; T-SICI = threshold changes in short-interval intracortical inhibition; MEP = motor-evoked potential; RMT = resting motor threshold. Please click here to view a larger version of this figure.
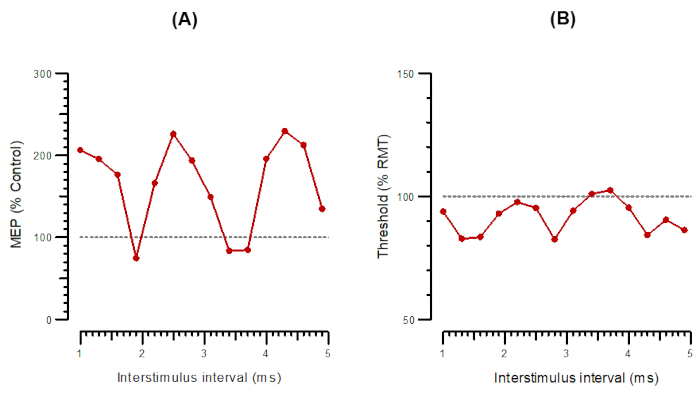
Figure 4: A-SICF and T-SICF plotted as a function of interstimulus intervals from 1 ms to 4.9 ms. (A) A-SICF plotted as the amplitude of conditioned response as a percentage of control. (B) T-SICF plotted as threshold changes (inhibition as a percentage of control). Abbreviations: A-SICF = amplitude of short-interval intracortical facilitation; T-SICF = threshold changes in short-interval intracortical facilitation; MEP = motor-evoked potential; RMT = resting motor threshold. Please click here to view a larger version of this figure.
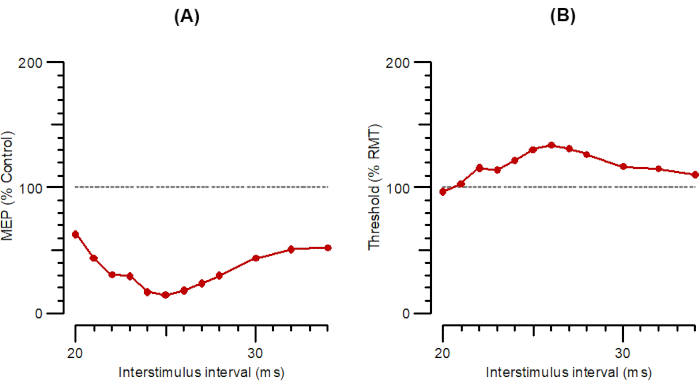
Figure 5: A-SAI and T-SAI plotted as a function of interstimulus intervals from 20 ms to 35 ms. (A) A-SAI plotted as the amplitude of conditioned response as a percentage of control. (B) T-SAI plotted as threshold changes (inhibition as a percentage of control). Abbreviations: A-SAI = amplitude of short-latency afferent inhibition; T-SAI = threshold changes in short-latency afferent inhibition; MEP = motor-evoked potential; RMT = resting motor threshold. Please click here to view a larger version of this figure.
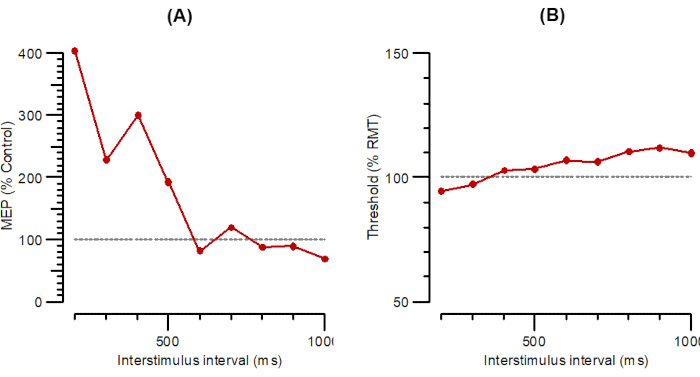
Figure 6: A-LAI and T-LAI plotted as a function of interstimulus intervals from 200 ms to 1000 ms. (A) A-LAI plotted as the amplitude of conditioned response as a percentage of control. (B) T-LAI plotted as threshold changes (inhibition as a percentage of control). Abbreviations: A-LAI = amplitude of long-latency afferent inhibition; T-LAI = threshold changes in long-latency afferent inhibition; MEP = motor-evoked potential; RMT = resting motor threshold. Please click here to view a larger version of this figure.
Table 1: The available TMS protocols in the software. Abbreviations: TMS = transcranial magnetic stimulation; SICI = Short interval intracortical inhibition; SICF = Short interval intracortical facilitation; LICI = Long interval intracortical inhibition; SAI = Short latency afferent inhibition; LAI = Long latency afferent inhibition; µV = microvolt. Please click here to download this Table.
