A total of 399 and 463 SitTS trials were completed without and with FES assisted correspondingly. The trials that contributed to each set are tabulated in Table 2. The participants could perform more SitTS trials with the presence of electrical stimulation on their legs, i.e., FES. Overall, both participants managed to perform more SitTS trials with the aid of FES. This suggests that FES helps in stimulating participants' quadriceps to execute SitTS action in a prolonged period20. There were three phases of SitTS described in this study. Phase 1 began with the start of the movement and lasted when the buttocks left the seat. Phase 2 referred to the time when buttocks leave the seat up to the maximum hip flexion event. Phase 3 denoted from the beginning of hip extension and lasted until the end of the movement. Each phase contributed 23% ± 7% for Phase 1, 16% ± 4% for Phase 2, and 61% ± 6% for Phase 3 of the SitTS cycle, as illustrated in Figure 3. Three phases of SitTS were defined in this study following an earlier study by Kagaya et al. that had a similar protocol of exercise in which SCI participants used the aid of hand-assists21. Phase 1 displayed the highest standard deviation (SD) of its contribution with ±7% proving that participants recruit diverse strategies to initiate buttocks lift-up from the seat throughout the study.
Overall, the mean time of FES-SitTS cycle between the initial trial in each set was identified to be significantly shorter (t = 1.28 s) as compared to the final trials (t = 1.66 s) in each set (p < 0.0005), as shown in Table 3. This indicates slower standing-up movement, most likely due to muscle tiredness or fatigue, and the added effort to stabilize themselves during the standing-up movement. FES-evoked exercise caused participants to be more prone to fatigue towards the end of their SitTS action in each set. Meanwhile, a non-significant difference of mean time was observed during voluntary SitTS activity p = 0.571, which suggests that there are several strategies of SitTS accomplishment initiated by participants throughout the voluntary SitTS session. There were some factors that might contribute to these several strategies, which consumed diverse time allocation. Participants' feet placement22,23 and trunk control22 during the early phase of voluntary SitTS played a major contribution as there were a few times participants tended to lift one of the feet and sway their trunk from front to back24 first before they started leaving the chair. This is also associated with the previous study by Lee & Lee24 that investigated the forward-and-backward swaying in preparation to stand was affected by the height of the chair.
The presence of negative values at the leg% during the early to middle stage of SitTS (Figure 4A, Figure 5A, Figure 6A, and Figure 7A) were due to the calibration procedure of force plate 2 that was taken while participants' feet were in contact with these force plate. This initialized the stationary sitting force as zero, as their legs were lifted slightly when repositioning in preparation to stand, resulting in the force value appearing negative. Since both participants had the pattern of adjusting their feet position by lifting the leg during the early stage of SitTS, force plate 2 showed a negative magnitude of force which indicated the eliminated force that existed by the feet before the calibration process took place. The habit of adjusting their feet position before actually standing might be a common practice of biomechanical preparation among all, which needs to be considered in other standing-related exercises25. Similarly, Camargos et al. reported that patients need to adopt a spontaneous SitTS strategy which results in higher functional levels25. Additionally, normalized root mean square (RMS)-MMG exhibited a similar graph pattern throughout the study. The amplitude of RMS-MMG was correlated to quadriceps muscle contraction and its force production26. The highest peak amplitude of normalized RMS-MMG described that the quadriceps muscles produced the highest force in between Phase 1 and Phase 2 of SitTS cycle (Figure 4C, Figure 5C, Figure 6C, and Figure 7C ). These highest forces were generated by the participants to prepare their legs for early knee joint stabilization before its extension. In addition, quadriceps muscles were observed to produce greater muscle contraction during the late phase of SitTS to help the legs to stabilize the feet and legs for standing posture22,25.
Furthermore, muscle contraction at the right leg was significantly higher as compared to the left leg for both participants during voluntary SitTS action (p < 0.05). These voluntary SitTS allowed them to use all strength from their limbs, especially from their legs, to execute the SitTS action. Hence both participants were assumed to use more effort on the right leg during these actions. In addition, Participant 1 had contracture of the right quadriceps muscle, which resulted in continuous contraction, thereby generating constant muscle force throughout the experiment.
Meanwhile, Table 4 summarises the answers given by the participants regarding their experience in performing the SitTS exercise. The contribution of arms and legs during SitTS movement varied among the participants based on their MRC muscle strength grade. In this study, the lower limbs' muscle strength for each participant is accessible in step 1.1.2. Hence in this step, the SCI participants' arms and legs contributions are presented individually, as shown in Figure 4 para Figure 7.
Biomechanical contributions of arms versus legs
Overall, throughout the SitTS action in both sessions, Participant 1's arm percentage showed a higher contribution in total body weight percentage as compared to his leg percentage (Figure 4A and Figure 5A). This result occurred as Participant 1 completely utilized his strength in both arms and left legs to bring up his upper body for standing. Both arms were used to support the left leg in providing stability for the whole body. Therefore, he endured most of his body weight using the arms and SF during the accomplishment of SitTS. Participant 1 had several joint contractures in the right knee and right ankle of the leg. As a result, Participant 1 did not put his body weight onto the right leg during the exercise. By comparing the two sessions, a higher contribution of Participant 1's arm percentage was presented during FES SitTS. This result proposes that his arms were utilized to control a full right knee extension that was stimulated by FES. Even though the muscles were electrically-stimulated in Participant 1, his right knee could not provide full knee extension during the end phase of SitTS. This statement is validated as the right knee angle did not reach normal knee extension range of motion (0° to 5°) during late phase of SitTS, as shown in Figure 4B and Figure 5B.
For Participant 2, there were huge increases of leg percentage from Phase 2 to Phase 3 of SitTS in both sessions. In general, Participant 2 had a better score of MRC muscle grade for legs as compared to Participant 1. As a result, Participant 2's arms and legs contribution pattern changed drastically throughout the SitTS action. Towards the end of the SitTS cycle, Participant 2's legs contributed 79.5% (without FES) and 78.8% (with FES) of the load-bearing, proving that her legs provided good weight-bearing to support her whole body during standing. The results suggested that the arms play a minor role in assisting Participant 2 during SitTS study.
In contrast, by comparing 2 sessions (Figure 6A and Figure 7A), a higher contribution of leg% during the end phase of voluntary SitTS proposed that Participant 2 exerted more strength onto her legs to bear the full body weight. In addition, during the final set of voluntary SitTS, Participant 2 exhibited a smaller knee angle during the early stage of the movement (Figure 6B). This finding suggests that towards the final set of voluntary SitTS tasks, Participant 2 compensated her fatigued state by positioning a smaller knee angle that provided lesser pressure on the feet27. In addition, FES stimulation helped Participant 2 perform SitTS by giving less strength exertion to the legs at the force plate during the end phase of session 2.
Subjective feedback
Among the 3 phases, which included 5 events of SitTS (Figure 3), both participants reported that their arms were the most tired during Event B while their legs were most tired during Event C. These 2 events were closely related to each other as both events occurred at Phase 2 of the SitTS motion. During Event B, i.e., when the buttocks lift-up was initiated, Participant 1 was observed to increase arm strength to lift his upper body from the chair (Figure 4A and Figure 5A). Meanwhile for Participant 2, the maximum contribution of arms was detected during Event B for FES-assisted SitTS (Figure 7A). These coincided with the accomplishment of SitTS action that was continued with the preparation of legs to stand without falling during Event C as observed by the motion analysis system (Figure 4B, Figure 5B, Figure 6B, and Figure 7B). These assumptions were verified as both participants' knee angles started to decrease (knee started to extend). These ideas are supported by participants' opinions during the interview. Participant 2 selected Event A in both conditions as the most stable position. The answer given by Participant 2 was expected as she felt secure while sitting on the chair.
Conversely, without the help of FES, Participant 1 felt most stable during Event C. This result was due to the presence of arm strength that assisted him to carry his body weight upward. While with the aid of FES, Event E was chosen as the most stable as he agreed that FES had helped him to straighten both his knees and allowed him to stand up confidently. Besides that, Participant 1 experienced the least stable position at Event E during voluntary SitTS due to his weak right leg (Quadriceps MRC muscle grade: Grade 2). These statements were proven by his major arms contribution towards the end of SitTS phase, as illustrated biomechanically in Figure 4A and Figure 5A. Next, with the aid of FES, Participant 1 felt the least stable during Event B, as reflected in Figure 3. Even with the presence of FES, Participant 1 believed that these events were where the initial transition of his body moving from sitting to standing. Meanwhile, Participant 2 felt the least stable during Event C in both sessions. These corresponded with the arrangement of both legs and arms to stand without falling as observed by the motion analysis system and illustrated in Figure 6 and Figure 7. The verbal expression was biomechanically verified as Participant 2's knee started to fully extend (Figure 6B and Figure 7B).
In addition, the normalized RMS-MMG of the quadriceps muscle showed a peak value during Event C. This indicated his effort to straighten his body to increase the hip angle when standing. Additionally, during the final trial of FES assisted SitTS session (Figure 7C), both quadriceps muscles displayed a small constant normalized RMS-MMG value throughout SitTS phase as agreed by Participant 2, who already felt tired, which emphasized the point of using the upper body to straighten herself in the final few standing process. In addition, following the FES-assisted SitTS session, both participants were confident with the use of FES device. Overall, participants experienced positive outcomes during their exercise.
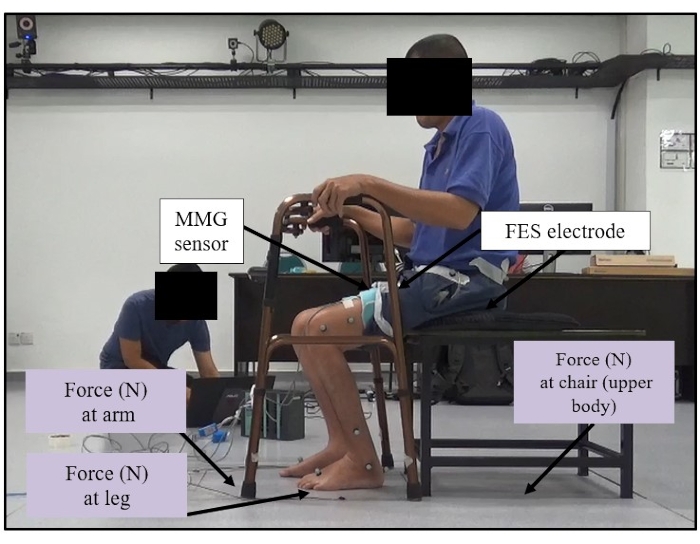
Figure 1: Custom-made chair setup. The custom-made chair was placed inside force plate 1. Both feet were placed on force plate 2. This figure shows the overall setup of the participant's initial position on the custom-made chair and instrumented SF with the force plates. Please click here to view a larger version of this figure.
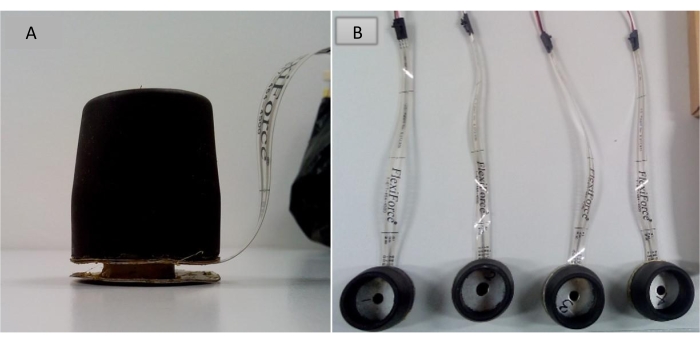
Figure 2: Placement of the force sensor. (A) An instrumented force sensor was placed at the bottom part of the rubber stopper of SF (side view). (B) The placement of four instrumented force sensors (top view). The figure presents the placement of the force sensor at the bottom part of the rubber stopper of the SF. Please click here to view a larger version of this figure.
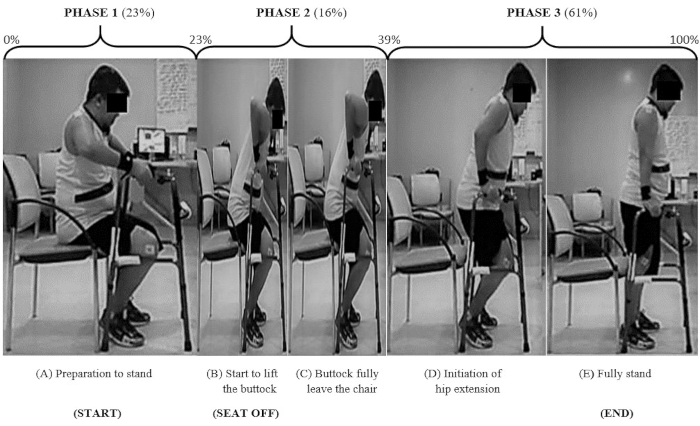
Figure 3: A cycle of SitTS activity assisted by SF. The figure describes a complete cycle of SitTS with the presence of a standing frame. Please click here to view a larger version of this figure.
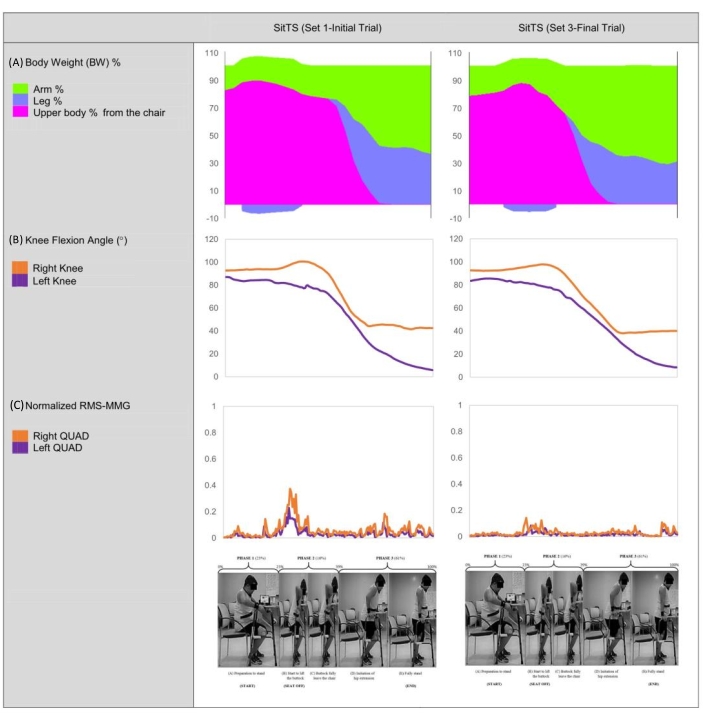
Figure 4: Participant 1's body weight contribution, knee flexion angle, and normalized quadriceps RMS-MMG during voluntary SitTS (Set 1-Initial Trial versus Set 3-Final Trial). The figure illustrates the parameters obtained by Participant 1 during the voluntary SitTS exercise. Please click here to view a larger version of this figure.
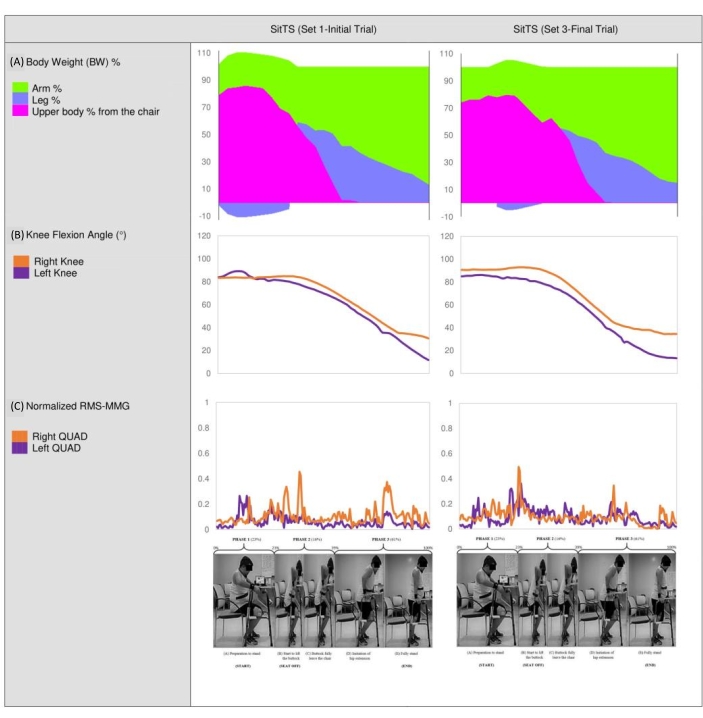
Figure 5: Participant 1's body weight contribution, knee flexion angle, and normalized quadriceps RMS-MMG during assisted FES SitTS (Set 1-Initial Trial versus Set 3-Final Trial). The figure explains the parameters obtained by Participant 1 during FES assisted SitTS exercise. Please click here to view a larger version of this figure.
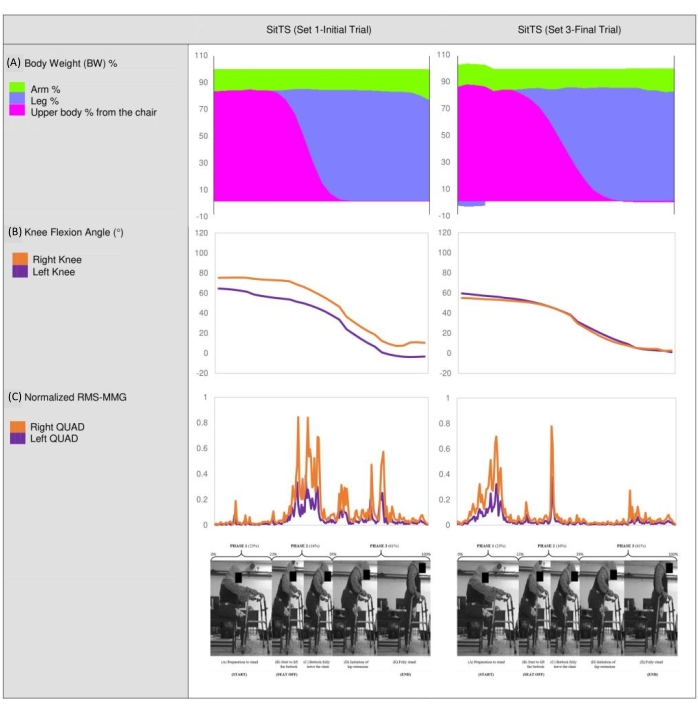
Figure 6: Participant 2's body weight contribution, knee flexion angle, and normalized quadriceps RMS-MMG during voluntary SitTS (Set 1-Initial Trial versus Set 3-Final Trial). The figure illustrates the parameters obtained by Participant 2 during the voluntary SitTS exercise. Please click here to view a larger version of this figure.
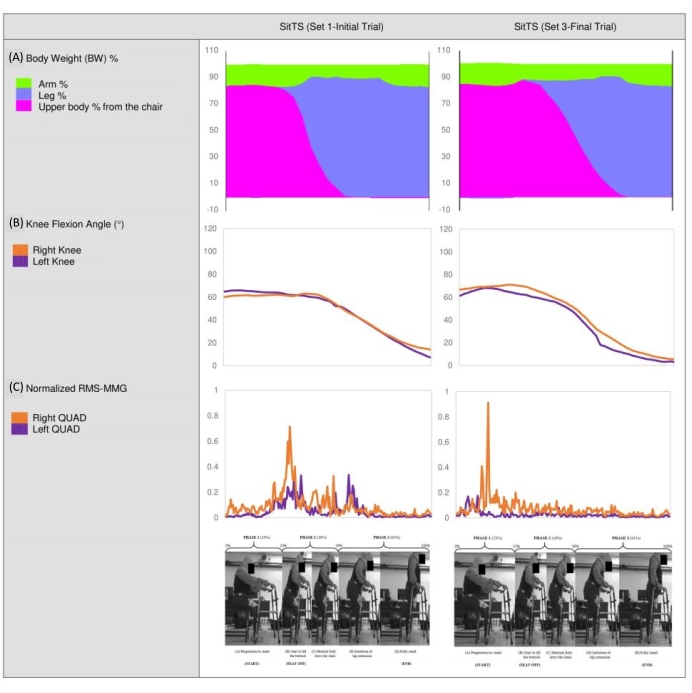
Figure 7: Participant 2's body weight contribution, knee flexion angle, and normalized quadriceps RMS-MMG during assisted FES SitTS (Set 1-Initial Trial versus Set 3-Final Trial). The figure explains the parameters obtained by Participant 2 during FES assisted SitTS exercise. Please click here to view a larger version of this figure.
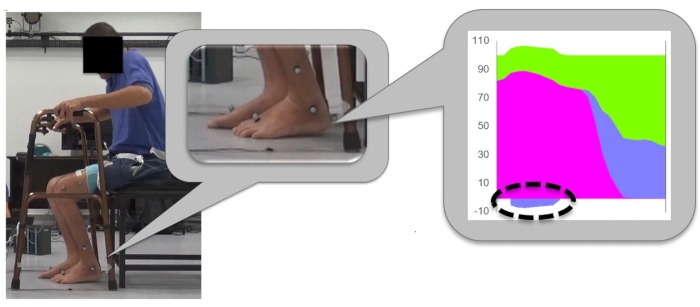
Figure 8: The condition of SCI participants lifting the leg hence producing the negative value of the legs force during the early phase of SitTS. The figure verifies the negative value obtains from the legs' force when participant tries to lift the heel during the initial phase of SitTS. Please click here to view a larger version of this figure.
Figure 9: The combination of the determinants in the SitTS experiment. The figure concludes the combined parameters involved in the SitTS study. Please click here to view a larger version of this figure.
| Participant | Leg | FES current (mA) | |
| Quadriceps | Gluteal Maximus | ||
| 1 | R | 58 | 46 |
| L | 46 | 46 | |
| 2 | R | 35 | 28 |
| L | 35 | 28 | |
Table 1: FES current stimulated during SitTS study. The table shows the amplitude of FES current for each participant on the quadriceps and gluteal maximus muscle.
| Participant | Number of SitTS trials | |||||
| No FES | FES | |||||
| Set 1 | Set 2 | Set 3 | Set 1 | Set 2 | Set 3 | |
| 1 | 96 | 30 | 31 | 96 | 61 | 36 |
| 2 | 95 | 92 | 55 | 89 | 91 | 90 |
Table 2: Number of completed trials of SitTS movements by two SCI individuals. The table provides the total number of SitTS trials by the participants.
| Trials | N | No FES | FES |
| Mean time (s) | Mean time (s) | ||
| Initial | 60 | 1.57 ± 0.244 | 1.28 ± 0.123a |
| Final | 60 | 1.84 ± 0.210 | 1.66 ± 0.295a |
Table 3: Mean time for a complete cycle of SitTS during initial and final trials in each set. The table presents the mean time taken for participants to complete a cycle of SitTS during initial and final trials in each set. An independent sample t-test was done, values were given as mean ± SD (N = 60). Means with superscripts 'a' were significant (p < 0.0005).
| Participant 1 | Participant 2 | ||||||
| Without FES | With FES | Without FES | With FES | ||||
| Which event(s) do you think is the most tiring for your upper limbs? | B | B | B | B | |||
| Which event(s) do you think is the most tiring for your lower limbs? | C | C | C | C | |||
| Which event(s) do you think is the most stable during experiment? | C | E | A | A | |||
| Which event(s) do you think is the least stable during experiment | E | B | C | C | |||
Table 4: Reported stability and fatigue experienced by participants during the accomplishment of SitTS activity. The table shows the answer given by participants regarding their stability and fatigue experienced during SitTS exercise.
