The quantitative variables are expressed as mean ± standard error of the mean (SEM). Except for the comparison of IOP dynamics between OHT and control groups (Figure 1F), statistical analysis was performed using two-way ANOVA followed by Sidak's multiple comparisons test. A p-value < 0.05 was considered statistically significant.
Figure 1 illustrates surgical steps of the full-circle limbal plexus cauterization (LPC) model, with important landmarks such as 360° thermal-induced disappearance of limbal vessels, as well as the mild to moderate mydriasis in the operated eye at the end of the procedure.
In the present series of 131 rats, full-circle limbal plexus cauterization (LPC) induced IOP elevation immediately after surgery from 13.0 ± 0.2 mmHg at baseline to 22.7 ± 0.4 mmHg. Peak postoperative IOP was observed on the first day after surgery (25.3 ± 0.6 mmHg), followed by a gradual return to baseline levels at the 6th postoperative day (statistical analysis: multiple t-test corrected for multiple comparisons using the Holm-Sidak method; Figure 1F). Corneal fibrosis or edema were clinical intercurrences that could potentially compromise accurate IOP measurement. The first, on one hand, was rare, affecting 3.92% of animals and noticed late during the postoperative follow-up, thus sparing the first 5 days of ocular hypertension and preserving the subacute OHT profile described23. Corneal edema, on the other hand, was a more common complication seen during the first few days after surgery (1-3 days), but mostly mild and temporary, thus did not robustly affect IOP23.
Retinal function was evaluated both behaviorally and electrophysiologically using the optomotor reflex and pattern-ERG, respectively (Figure 1G–J). Both parameters showed two phases of impairment: an ocular hypertension acute phase at 3rd day post-surgery, and a secondary degeneration phase at the 30th day post-surgery (Figure 1H, Figure J, and Table 1). In between, a period of functional recovery was detected, as previously discussed elsewhere23.
Compared with control fellow optic nerves, axonal counts in semi-thin transversal optic nerve sections showed progressive decrease after surgery (3rd day: 68.3% ± 0.9%; 7th day: 59.2% ± 2.6%; 14th day: 45.4% ± 2.2%; 30th day: 28.2 % ± 3.0%; two-way ANOVA: p < 0.0001; Figure 2A). Ultra-structurally, optic nerves from control eyes presented densely packed myelinated fibers, separated by thin glial cells processes, and evident axonal microtubules and neurofilaments (Figure 2B). In contrast, at 3 days after OHT, we found focal disruption of axon bundles, a few degenerated fibers, cytoplasmic vacuolation in glial cells processes, and condensed chromatin in glial cell nuclei. After 7 days of OHT induction, there was an increase in degenerated axonal fibers, hypertrophic glial cell processes, and swelling and voids in individual axonal fibers. At 14 days, one of the most prominent changes was a greater disarrangement of the optic nerve fibers, associated with the invasion of glial cell processes among the axons. Filament bundles filled these processes and dark degenerated fibers, and myelin breakdown was more common, associated with detached and vacuolized lamellae (Figure 2B).
The density of Brn3a+ profiles decreased along time (Figure 2C), mainly in the dorsal and temporal retinal quadrants, down to 32.4% ± 9.6% and 35.7% ± 9.1% after 30 days, respectively (Figures 2D–G and Table 2).
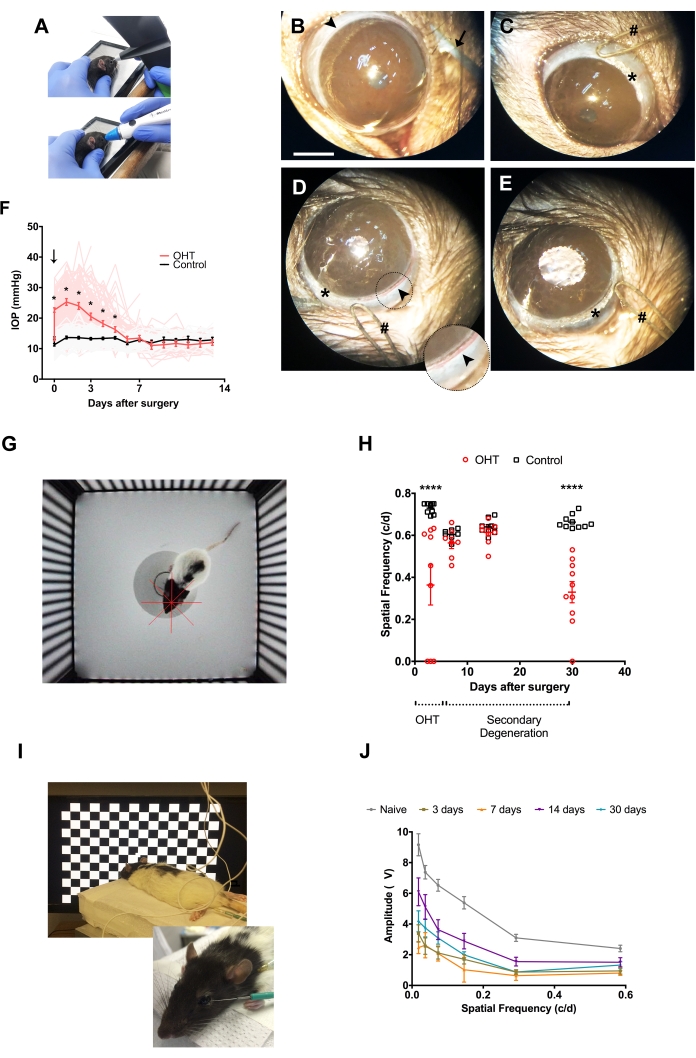
Figure 1: Thermal cauterization of limbal vascular plexus and consequences to retinal function in vivo. (A) Alternative methods to measure IOP in rats: rebound tonometry (superior), and applanation tonometry (inferior). (B–E) Surgical procedure; arrowhead: limbal vascular plexus; arrow: curved forceps used to expose anterior surface of the eyeball and optimize surgical assessment to limbal vessels; hash: the round tip of the low-temperature ophthalmic cautery; asterisk: cauterization mark. Scale bar: 2 mm. Inset in (D) shows in higher magnification the limbal vasculature to be cauterized. (F) Time course of IOP measurements in OHT (red) and control (black) eyes (n = 131). Vertical downward arrow: LPC surgery. * = p < 0.05 (G) Arena for optomotor response analysis, comprised of four computer monitors arranged in a quadrangle, with a platform in the middle. The monitors display the image of a virtual cylinder composed of vertical alternate black and white stripes moving around the animal with constant rotational speed and variable spatial frequencies. The red crosshair corresponds to the center of the virtual cylinder. (H) Optomotor responses. Two distinct phases are distinguished upon surgical follow-up: the OHT phase (0-5 days) and the secondary degeneration phase (6-30 days). **** = p < 0.0001. (I) Electrodes and animal positioning for pattern-ERG (PERG) acquisition: the active electrode at the temporal periphery of the cornea, and the reference and ground electrodes into the subcutaneous tissue of the ipsilateral temporal canthus and one of the hind limbs, respectively. The animal is positioned at 20 cm from the stimulus screen. (J) PERG amplitude upon stimuli with different spatial frequencies. Similar to optomotor response, PERG evaluation also shows two distinct phases of responses after surgery: ocular hypertensive at 3 days post-surgery, followed by recovery at day 7 and 14, although still statistically lower than naïve responses, and a subsequent decrease at day 30 after surgery. c/d = cycles per degree. Naïve group: eyes of animals unexposed to any previous experimental manipulation. (H) and (J) show mean ± SEM, plus individual replicates in (H). Please click here to view a larger version of this figure.
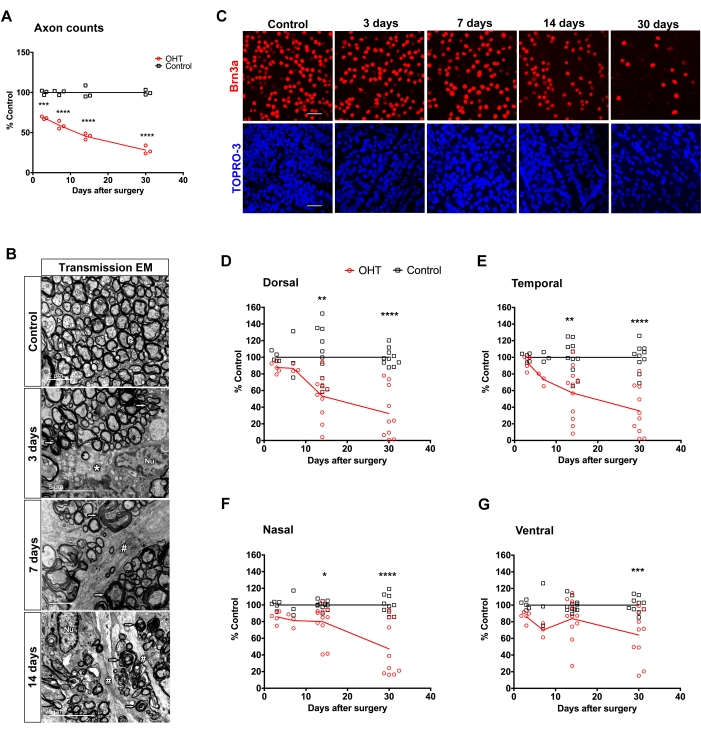
Figure 2: Structural assessment of retina and optic nerve after limbal vascular plexus cauterization (LPC) with low-temperature ophthalmic cautery. (A) Axon counts at distinct times after OHT (n = 3). *** = p = 0.0005, **** = p < 0.0001. (B) Electron micrographs of optic nerve degeneration following OHT. The left image shows the control optic nerve, and the following images illustrate the progressive degeneration after 3, 7, and 14 days of OHT. Arrowhead: normal myelinated fibers; thin arrows: degenerated fibers; asterisk: cytoplasmic vacuolation; hashes: glial cells process; and Nu: glial cell nucleus. (C) Photomicrographs of representative counting fields of RGCs labeled with an antibody to Brn3a (red) and TO-PRO3 labeled nuclei (blue); scale bar: 50µm. (D–G) Distribution of average Brn3a+ cell density in the four quadrants of the retina after 3-30 days of surgery. The graphs show individual averages of RGC densities for 3-11 animals per time after the procedure. * = p < 0.05; ** = p < 0.01; *** = p < 0.001; **** = p < 0.0001. Quantitative data is mean ± SEM. Please click here to view a larger version of this figure.
Table 1: Statistical analysis of PERG data. Two-way ANOVA followed by Sidak's multiple comparisons test. P-value less than 0.05 was considered statistically significant. c/d = cycles per degree. Please click here to download this Table.
Table 2: Regional loss of RGC after LPC. SEM: standard error of the mean. Control: fellow eye. P-values less than 0.05 were considered statistically significant (*). Please click here to download this Table.
