Female mice have five pairs of mammary glands with a single ductal tree that opens at the nipple orifice22. At the tips of the developing ductal tree are the terminal end buds (TEBs), proliferative structures that direct growth and branching. After puberty when the elongation phase is completed, TEBs regress and become functionally and anatomically indistinguishable from terminal ducts or alveolar buds23. Terminal ductal lobular units serve a similar function in humans as TEBs do in mice and are the sites from which breast cancer predominantly arises24,25. We can inject up to 50 μL of 70% EtOH solution to fill the entire ductal tree of thoracic and abdominal mammary glands of 9-week-old FVB/N, NSG, and other mouse strains (Figure 1, Figure 2, Figure 3, see references3,16). In a typical experiment, we can inject up to eight mammary glands with an ablative solution of 70% EtOH and 100 mM TaOx in two consecutive ID procedures separated by 7 days to allow for animal recovery (Figure 2). Animals are imaged by micro-CT immediately after the last ID injection to assess successful delivery of the solution to the entire ductal tree (Figure 2). In our experience, the nipples of inguinal glands are suitable for injection in about 60% of the animals, and the nipples of cervical glands in about 40%. When suitable, we can inject up to 30 μL of 70% EtOH solution to fill the entire ductal tree of cervical and inguinal mammary glands (Figure 2). FVB and NSG strains generally present more suitable nipples for injection than C57BL/6J or mixed genetic background strains. Whole mount dual staining protocol or 3D confocal microscopy are good orthogonal methods to confirm to what extent the ductal tree was filled (Figure 3). These tissue-correlate analyses are compatible with and can be performed after in vivo imaging. The obvious limitation of these orthogonal methods is that they require animal termination for tissue collection and analysis; however, in an optimization phase of a new ablative formulation, they provide independent validation.
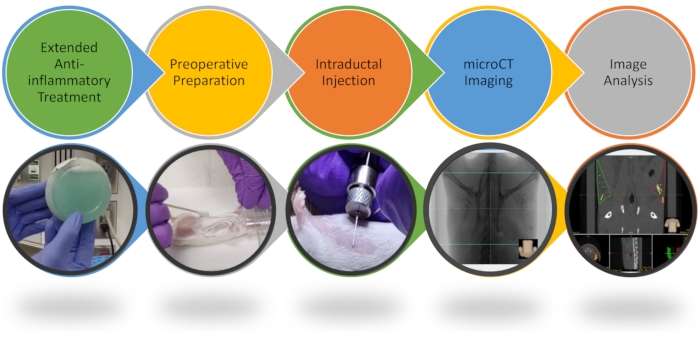
Figure 1: Workflow of intraductal procedure and image analysis. Key steps of the ID procedure are highlighted. Please see the video for more details. Please click here to view a larger version of this figure.
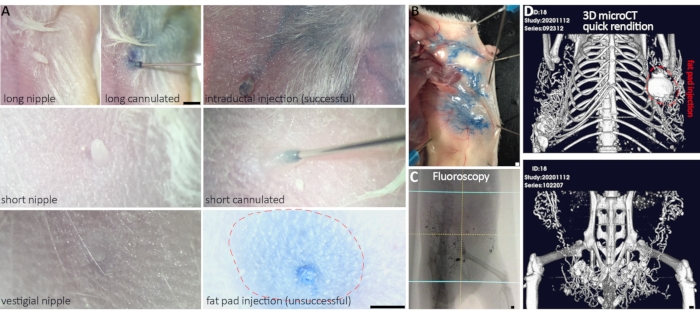
Figure 2: Successful cannulation and delivery of ablative solution to multiple mammary glands. (A) Representative nipple variegation in FVB and NSG mouse strains. Long nipples are easier to cannulate than short nipples, whereas too short or vestigial nipples cannot be cannulated. Once cannulated, the size of the nipple does not affect successful intraductal delivery. (B) Gross anatomical analysis of blue dye in an ablative solution provides ex vivo evidence of ductal tree filling and delivery success. (C,D) Real-time fluoroscopy and post-image acquisition 3D micro-CT rendition provide in vivo evidence of delivery success. (D) Successful injection of both abdominal and inguinal glands, and three out of four thoracic glands (fat pad injection in gland #2). Scale bars correspond to 1 mm in images at different magnification. Please click here to view a larger version of this figure.
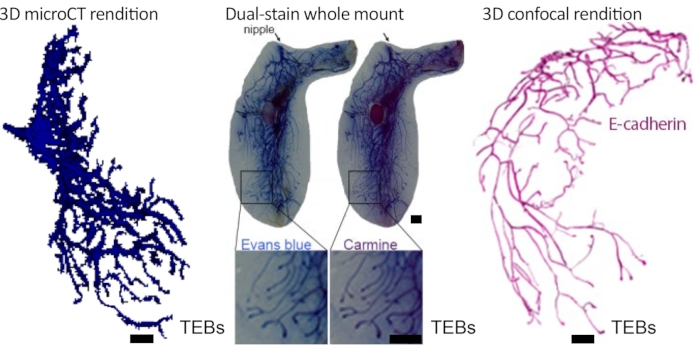
Figure 3: In vivo and ex vivo demonstration of ductal tree filling. 70% EtOH/100 mM TaOx nanoparticles/Evans Blue solution was intraductally injected into the mouse abdominal mammary gland and immediately imaged by micro-CT and processed for dual whole mount staining. Ductal tree was reconstructed using an image analysis software package. The solution entirely fills the carmine alum-stained ductal tree. A separate gland was immunostained for E-Cadherin (Cdh1), cleared using Benzyl Alcohol:Benzyl Benzoate and imaged by confocal microscopy as described26. The ductal tree was reconstructed using image analysis software. Pseudo-coloring rendering of confocal image (i.e., black background to white, green marker signal to magenta) was obtained with the image invert function of the image editing software. Scale bars correspond to 1 mm in images at different magnification. This figure has been modified from reference no.3. Please click here to view a larger version of this figure.
| Issue | Appearance | Solution | |||
| Short nipple (Fig. 2) | Nipple has low profile – hard to grab | It is sometimes easier to hold the skin near the nipple and target the center of the nipple with the needle. The needle will likely dive under the skin. Pulling up slowly may reveal the nipple to be slightly over the tip of the needle and give room to grab and pull it the rest of the way onto the needle. Be very careful when diving below the skin about the angle of the needle. It is easy to inadvertently get a fat pad injection by stabbing at the wrong angle. | |||
| Fat nipple | Much larger than other nipples with little peelable dead skin – easily visible without scope | Very easy to get a fat pad injection on these nipples. Be very cautious about angle of the needle when inserting into nipple. | |||
| Fat pad injection (Fig. 2) | Swollen around nipple and possibly in nipple itself – easiest to see if color is added to injection solution | If nipple is swelling with first few ul injected, remove needle, and attempt to insert again with more care taken of angle. Begin injection again and watch for further swelling. If swelling continues, abandon attempt. It is very rare to successfully inject a nipple that has started out as a fat pad injection. | |||
| Wounds/scabbing | Open wound or scabbing near injection site of EtOH solution | Apply triple antibiotic ointment to open wounds but leave scabbed wounds alone. Applying ointment to scabs can increase likelihood animal will bother the scab and remove it. Check every 1-2 days until healed depending on severity of wound. Carprofen should be given until healed even if beyond normal window. | |||
Table 1: Troubleshooting and helpful tips.
