In this mouse cervical heterotopic heart transplantation model, the survival rate of recipient mice was approximately 95.2% (20 out of 21 mice survived). The primary cause of death was postoperative bleeding. The fast heartbeat with a regular rhythm serves as an indicator of the survival of the implanted donor heart.
C57BL/6 and BALB/c mice were MHC (H-2b) and MHC (H-2d) types in this model, respectively7,8. These two strains differ by the H-2, which causes acute T-cell-mediated rejection9. Of all the cardiac allografts, 62.5% were lost within 7 days after transplantation, as assessed by palpating the heartbeat. All cardiac allografts were lost within 8 days after transplantation. In contrast, all the isogeneic heart transplants survived beyond 4 weeks (Figure 2). Mice that survived beyond 4 weeks were euthanized by CO2 inhalation.
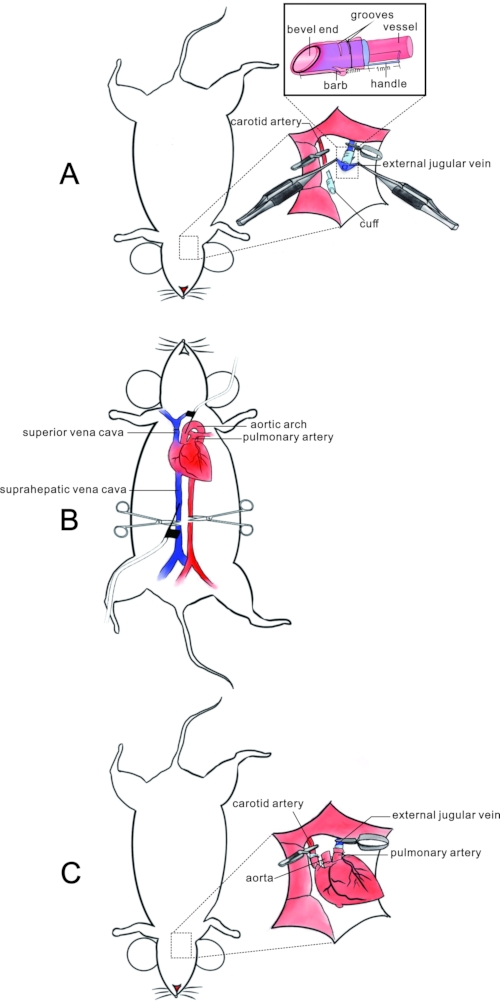
Figure 1: Schematic of the mouse cervical heterotopic heart transplantation model. (A) Protocol for preparing the recipient: after clipping the common carotid artery and external jugular vein at the proximal end, the vascular lumen of vessels is everted and fixed after passing through the barbed cuff with a bevel end and grooves on the surface. The dashed square shows the structure and usage of the cuff. (B) Donor heart resection: after the donor heart's perfusion with heparin and HTK solution from the inferior vena cava and aorta, the superior and inferior vena cava and pulmonary vein are ligated with sutures. The donor's heart is then resected by incising the vascular vessels. (C) Implantation of the donor's heart. The donor pulmonary artery and aorta is anastomosed to the recipient's external jugular vein, and carotid artery via the cuff with the recipient's vasculature turned inside out in an end-to-end pattern. Please click here to view a larger version of this figure.
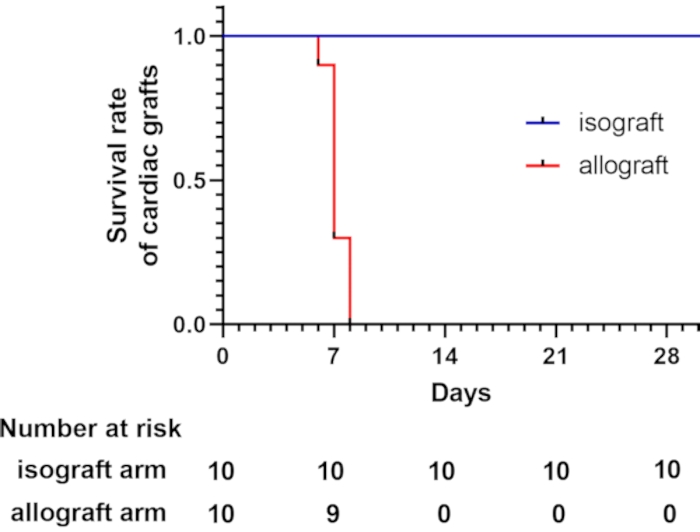
Figure 2: Survival curve for cardiac grafts. The survival curve of cardiac grafts shows that allogeneic heart transplants are lost within 8 days after transplantation, which was assessed by palpation of the heartbeat. A total of 10 recipient mice underwent the modified cervical heterotopic heart transplantation in each group. All the isogeneic heart transplants survived more than 4 weeks. Please click here to view a larger version of this figure.
| Rupert Oberhuber et al.10 | Xin Mao et al (present work) | |||
| Anaesthesia | xylazine and ketamine | isoflurane (Safe, continuous and stable) | ||
| Right lobe of the submandibular gland | removal | preservation (Reduce twirling of grafts) | ||
| Right sternocleidomastoid | removal | preservation (Reduce twirling of grafts) | ||
| Cardiac perfusion | Retrograde perfusion with 4 °C HTK solution from the aortic arch | 1. Anterograde perfusion with ice-cold physiological saline supplemented with 100 IU/mL heparin solution from the suprahepatic vena cava. 2. Retrograde reperfusion with ice-cold HTK solution from the aortic arch. (Reduce coagulation and increase myocardial protection) | ||
| Cuff | blunt end, with handle | bevel end, with handle, barb and grooves on the surface (Facilitate eversion and fixation) | ||
Table 1: Comparison of heart transplantation techniques. The current mouse cervical heterotopic heart transplantation technique is modified from Oberhuber, R. et al.10 and possesses additional advantages for cardiac graft survival.
