Following this protocol, 200,000 cryopreserved iBCs (previously confirmed to have a normal 46XY karyotype)11 were thawed and expanded in 3-D culture. Five days later, the resulting spheroids were dissociated, counted, and passaged again for further expansion. Approximately 480,000 cells were obtained and re-suspended in 3-D matrix (12 x 50 µL droplets, density 400 cells/µL). Fresh Basal Cell Medium was applied every 2-3 days. Ten days later, the cells were once again dissociated and counted. A total of 19.7 x 106 cells were harvested and prepared for FACS. 106 cells were stained with the APC-conjugated IgG1κ isotype control and the remaining 18.7 x 106 cells were stained with the APC-conjugated anti-NGFR antibody for 30 min protected from light (Figure 3).
NGFR+ gating was performed after comparison to the isotype control cells and was set purposely to collect the highest expressing NGFR+ cells (Figure 3). With this gating technique, 28% of live, single cells were NGFR+. While more cells were available, 750,000 cells were collected for downstream culture. Sorted cells were resuspended in Basal Cell Medium at a concentration of 50,000 cells/100 µL. 50,000 cells were then seeded onto each 6.5 mm porous membrane insert, which had been coated with human recombinant laminin-521 (2 µg/200 µL) per the manufacturer's guidelines. 500 µL Basal Cell Medium was added to the basolateral chamber of each insert and the plate was placed in a 37 °C humidified incubator. Three days later, the media in the apical chamber was aspirated and the cells were ~90% confluent by light microscopy (Figure 4B). The media from the basolateral chamber was aspirated; ALI Differentiation Medium was added to the apical (100 µL) and basolateral (500 µL) chambers. The next day, the media from the apical chamber was aspirated.
Over the following 21 days, the cells were evaluated by light microscopy periodically and fed with fresh ALI Differentiation Medium (basolateral chamber only) every 2-3 days. Individual cells were initially easily identifiable (Figure 4A), had an elongated and spindle-shaped appearance, and formed a loosely packed monolayer (Figure 4B). Over the subsequent days to weeks, the cells formed a tightly packed, highly cellular, epithelial layer, and after 7-10 days there was the clear emergence of beating cilia and mucus production. TEER of the samples were calculated and similar to primary cell controls (range from 700-1600 Ω x cm2)11. Subsequent fixation (day 21-28) with paraformaldehyde and immunolabeling for canonical airway epithelial cell markers was performed for MUC5AC and acetylated-α-tubulin, among others (Figure 4C). Overall, with our observation of motile cilia, mucus production as well as confirmatory immunostaining of multiciliated and secretory cells which is similar to that of primary HBECs, we concluded that we successfully generated airway epithelial cells from induced pluripotent stem cells.
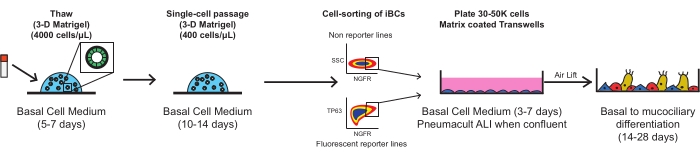
Figure 1: Overall schematic of protocol. Cryopreserved iBCs are thawed, expanded, and FACS purified prior to plating on porous membrane inserts, where they differentiate into a functional mucociliary epithelium. Please click here to view a larger version of this figure.
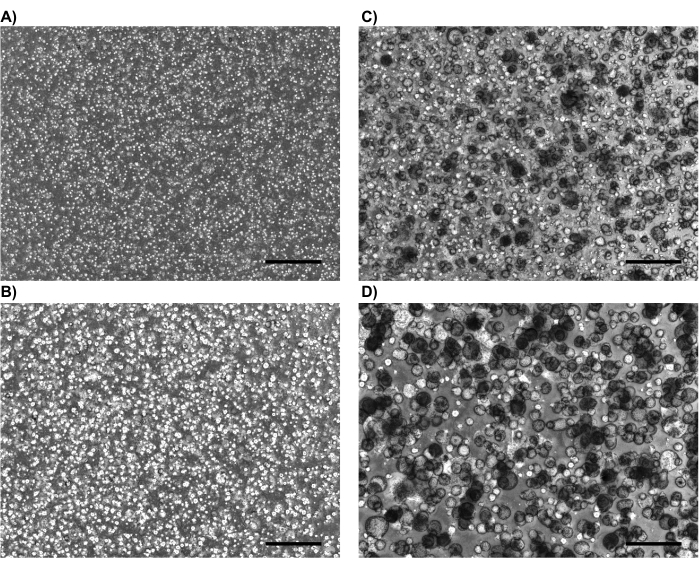
Figure 2: Representative phase contrast images. Representative phase contrast images demonstrating usual appearance of iBCs in 3-D culture after (A) 1 day, (B) 4 days, (C) 8 days, and (D) 14 days (just pre-NGFR sort). Scale bars represent 500 µm. Please click here to view a larger version of this figure.
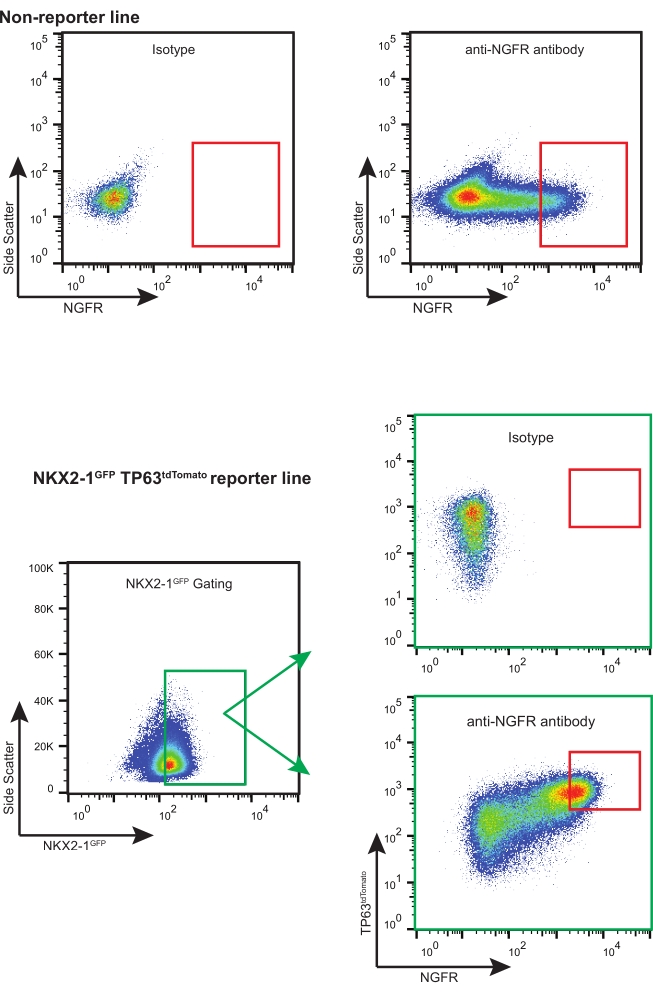
Figure 3: Representative FACS plots. Representative FACS plots for non-reporter and fluorescent-reporter iBCs. Examples of isotype controls are shown and were used to select for the highest expressing NGFR+ cells. Fluorescent reporter-containing iPSC lines are "triple sorted" for NKX2-1GFP+ TP63tdTomato+ NGFR+ cells. Please click here to view a larger version of this figure.
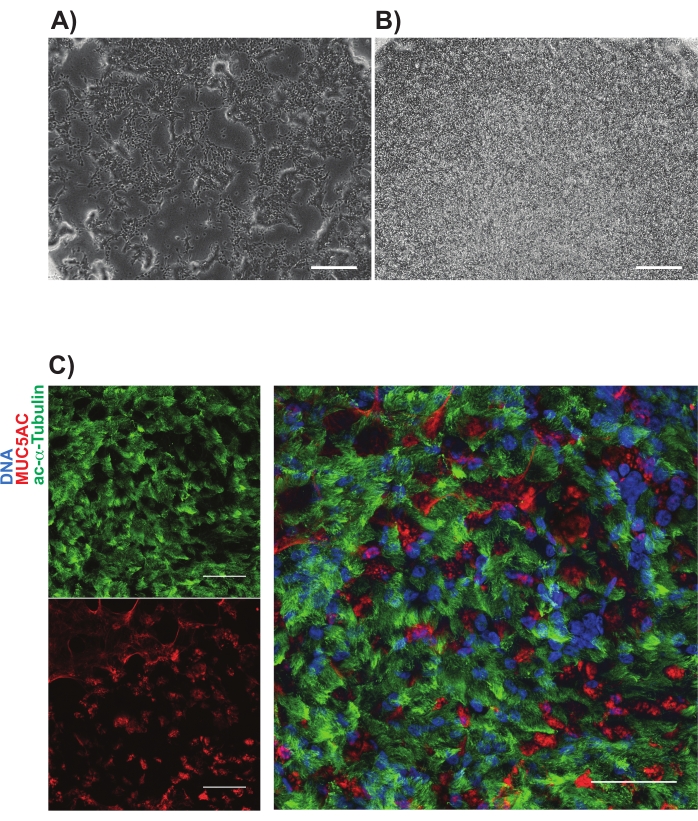
Figure 4: Representative images of iBC cultures on porous membranes. Phase contrast images are shown (A) 1 day and (B) 3 days after plating. Representative immunolabeling of mucociliary cultures shown in (C); acetylated-alpha tubulin (green) and MUC5AC (red). Scale bars represent 25 µm. Please click here to view a larger version of this figure.
Supplementary File 1: Media component table. Please click here to download this File.
