A total of 41 mice were used for this study. After three mortalities, one in MCAo and two in MCAo + EMS, a total of 38 mice were used for obtaining the results shown.
Estatística
Data from each experiment are presented as mean ± standard deviation (S.D.). Significance was determined using either unpaired student's t-test for comparing two groups or one-way ANOVA for more than two groups, with a Newman−Keuls post-hoc test to correct for multiple comparisons.
Nicotinamide adenine dinucleotide (reduced)-tetrazolium reductase (NADH-TR) staining
This staining was done to assess the long-term viability of the grafted muscle as in Turoczi et al.19. Briefly, at the time of sacrifice, the grafted muscle flap was carefully excised, fixed with 4% paraformaldehyde for 30 min, and cryopreserved in optimum cutting temperature (OCT) medium at -80 °C. Several 12 µm thick cryosections of temporalis muscle tissue were stained for NADH-TR enzyme-histochemical reaction. Slides were incubated for 30 min at 37 °C in a solution of nitroblue tetrazolium (1.8 mg/dL) and NADH (15 mg/dL) in 0.05 M Tris buffer (pH 7.6). Unused tetrazolium reagent was removed using increasing followed by decreasing concentrations of acetone. Quantitative assessment of NADH-tetrazolium-stained muscle was performed on muscle images taken at 40x magnification.
Immunostaining studies
Immunostaining was used to visualize muscle graft bonding with cortex and blood vessel density at the junction of muscle and cortex20,21. For visualization of muscle bonding with brain tissue, mice that had undergone EMS surgery were used here. At the end of each respective time point, mice were anesthetized with an avertin injection (50 mg/kg body weight), followed by perfusion with 1x PBS containing 5 mM Ethylenediaminetetraacetic acid (EDTA) and fixation with 4% paraformaldehyde. The skull was carefully cut to prevent accidental detachment of temporalis muscle (TM) graft from brain cortex. TM graft above the brain cortex was then separated from the remaining temporalis muscle. The brain was carefully removed and post-fixed in 4% paraformaldehyde overnight. The fixed brain was then dehydrated with 30% sucrose in 1x PBSuntil the brain sunk to the bottom of the vial (approximately 1-3 days). Tissue sections of 30 µm size were cut with freezing microtome and mounted on slides.
For immunostaining of blood vessels in the ipsilateral brain cortex, MCAo and MCAo + EMS mice were sacrificed, perfused, fixed, and processed as above. Brain slices of 30 µm size were sectioned on a freezing microtome and mounted on a glass side. Antigen retrieval was done using citrate buffer (pH 6.0) and sections were incubated with blocking buffer followed by incubation overnight with primary antibodies, anti-alpha skeletal muscle actin 1:200, and Lectin-Dy59421,22. Three coronal brain sections per mouse (n = 5 mice/group; total = 15 sections) were taken between 0.45 mm and 0.98 mm from bregma, stained, and visualized for quantification at 20x magnification at the junction of the ischemic core and penumbra regions. A blinded observer quantified lectin positive vessel density in the brain parenchyma using ImageJ software.
Muscle graft remains viable at 21 days after EMS
One prerequisite for success of this surgery is long-term viability of the grafted temporalis muscle. The TM graft showed transient damage of muscle cells at 7 days after surgery in grafted muscle vs. control muscle (71.32% muscle cell survival ± 16.64% vs. 97.19% ± 3.81%). However, this difference between grafted and the control muscle vanished, and muscles recovered completely 21 days after surgery (98.22% ± 3.965 vs. 96.87% ± 2.27%; Figure 2A).
Muscle grafts make loose bonds with brain tissue
Successful grafting of the temporalis muscle onto the brain cortex surface is a foremost requirement for the success of this model. In both the EMS + MCAo and EMS-only model, the temporalis muscle grafts adhered to the cortical surface 21 days after EMS, suggesting successful surgery, graft implantation, and bonding (Figure 1B and Figure 2B).
Blood vessel density increases in the perilesional cortex after EMS
Acute stroke leads to acute reduction in cerebral blood flow, impeded recruitment of collateral vessels, abnormal vascular sprouting, and dysfunctional angiogenesis, which contribute to poor stroke outcomes23. EMS significantly increases blood vessel surface area and integrated density in perilesional cortex after stroke (p < 0.05 vs. MCAo-only; Figure 3).
Analysis of angiogenic and neuromodulating proteins
A mouse angiogenesis array was used to compare expression of angiogenic and neuromodulating proteins 7 days and 21 days after MCAo in MCAo-only vs. MCAo + EMS mice as per manufacturer's instructions24. ImageJ software was used to quantify pixel density for each data point of the protein dot blot. Data were recorded as the ratio of the density of each analyzed protein to the averaged density of the standards for each blot.
Fibroblast growth factor (FGF)-acidic is upregulated and osteopontin is downregulated after EMS
Protein array results showed a significant increase in protein levels of FGF-acidic (0.677 ± 0.007 vs. 0.585 ± 0.014, p = 0.045), a potent angiogenic factor, and decrease in osteopontin levels, a multifunctional molecule expressed in inflammatory conditions (0.692 ± 0.007 vs. 0.758 ± 0.014, p = 0.048) in the MCAo + EMS group 21 days after stroke, suggesting improved angiogenesis and neuroprotection (Figure 4A).
Mortality outcomes for EMS after stroke
Both MCAo and EMS are invasive surgical techniques that may cause some mortality in mice. In this experiment, there was between 10%-11% mortality in mice 21 days after MCAo surgery, which is an accepted death rate for mice subjected to 60 min of MCAo14. Performing EMS on mice after MCAo did not increase mortality (Figure 4B) suggesting tolerance of EMS surgery even after MCAo.
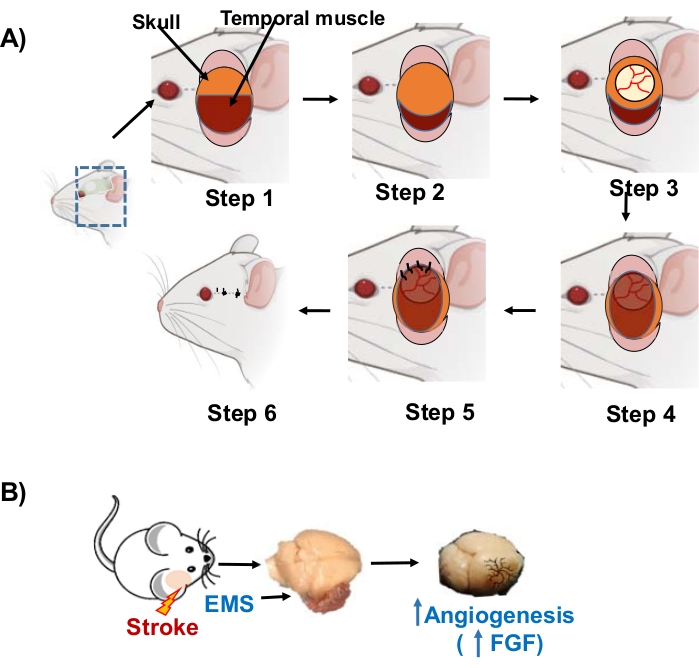
Figure 1. Stepwise EMS procedure after middle cerebral artery occlusion (MCAo): (A) Step 1. A skin incision is made over the right middle cerebral artery territory. The skin and subcutaneous tissues are reflected, exposing the skull and temporalis muscle. Step 2. The temporalis muscle is dissected away from the skull and reflected ventrally. Step 3. A craniotomy is performed (4-5 mm) and the dura is gently removed. Step 4. The temporalis muscle is placed directly on brain surface to cover the exposed cortex. Step 5. The dorsal edge of the temporalis muscle is sutured to the subcutaneous tissue of the dorsal skin flap, flush with the brain surface. Step 6. The incision is closed, and the mouse is removed from anesthesia and returned to its cage.This part of figure has been modified from25. (B) Conceptual schematic for encephalomyosynangiosis (EMS) treatment of MCAo-induced stroke. Abbreviations: FGF = Fibroblast growth factor. Please click here to view a larger version of this figure.
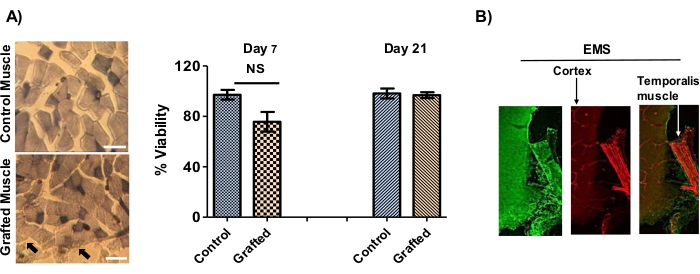
Figure 2. Immunostaining studies. (A) Temporalis muscle grafts maintain viability. Temporalis muscle grafts (EMS) on ischemic cortex tissue maintain high viability. (Left) Representative image of nicotinamide adenine dinucleotide (reduced)-tetrazolium reductase-stained muscle tissue cells from control (naïve muscle from contralateral side) and grafted muscle at 7 days after middle cerebral artery occlusion (MCAo) + encephalomyosynangiosis (EMS) surgery. Black arrow () shows damaged cells. (Right) Quantification of live/dead muscle cells. Muscle cells at 7 days after EMS show some mild damage (p < 0.1; t-test) that completely recovered at 21 days. (n = 5 mice/time points = total 10 mice in this group) Data are mean ± S.D. Scale bar = 20 µm. (B) Bonding of grafted temporalis muscle with brain cortex 21 days after EMS surgery. EMS tissues stained with anti-alpha skeletal muscle actin (green) and Lectin-Dy594 (red; blood vessel marker) antibody (n = 3 mice). Scale bar = 100 µm. Please click here to view a larger version of this figure.
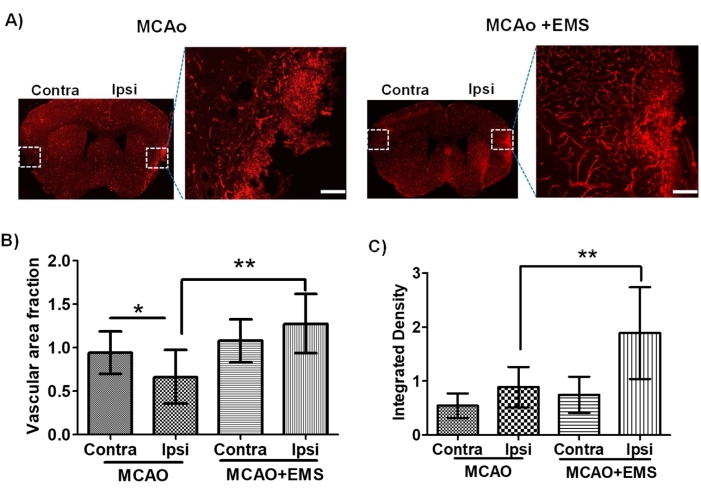
Figure 3: Encephalomyosynangiosis (EMS) surgery increases blood vessel density in ischemic lesions 21 days after stroke. (A) Representative images of coronal brain sections from mice subjected to (left) middle cerebral artery occlusion (MCAo) or (Right) MCAo + EMS and stained with L. esculentum (Tomato) Lectin-Dy594, which binds to glycoproteins in the basal membrane of endothelial cells. Graphs are quantified areas. MCAo + EMS mice showed higher endothelium network using parameters viz. vascular fraction area (B) and integrated density (C). **p < 0.01 (unpaired t-test), while MCAo-only mice showed damage close to the ischemic lesion (dashed line). N = 5 mice/group= 10 mice total. Data are mean ± S.D. Scale bar = 100 µm. Abbreviations: Contra = contralateral side; Ipsi =ipsilateral side. Please click here to view a larger version of this figure.
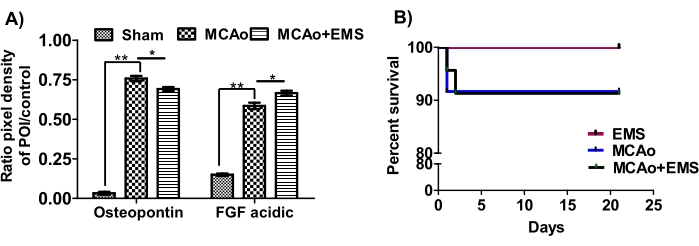
Figure 4: Encephalomyosynangiosis modulates angiogenic proteins after stroke. (A) A mouse angiogenesis array (ARY015) was used to simultaneously assess the relative levels of 53 mouse angiogenesis-related proteins after middle cerebral artery occlusion (MCAo) and MCAo + EMS (day 21 after MCAo) in brain tissue lysates from the perilesional cortex. Quantitative analysis shows that EMS surgery significantly reduced osteopontin and increased fibroblast growth factor (FGF)-acidic protein after stroke (*p < 0.05 or **p < 0.01) vs ipsilateral MCAo. Data are mean ± S.D.; n = 3 mice/group/time point = total 15 mice. (B) EMS did not increase mortality after stroke (MCAo). Kaplan Meier survival curve shows that EMS + MCAO did not change post-stroke mortality vs. MCAO alone (p = 0.54). For EMS n = 3; for MCAo n = 11; and for MCAo + EMS n = 21. Please click here to view a larger version of this figure.
