Results from two groups of rats are presented. UTx was carried out before (group 1, n = 8) and after (group 2, n = 8) protocol adjustment (Table 1) to demonstrate the effects of our modifications (please see the Discussion for an explanation of our modifications)12,15,21.
The outcome of rat UTx is associated with three key phases. The first phase is successful recovery from UTx. Usually, recipients should recover within the first 2 postoperative days. The second phase relates to the health status of the graft 2 weeks after surgery, which decides the inclusion into the mating process (Table 2). The third phase involves spontaneous mating followed by successful birth as evidence of fertility.
All animals from both groups had an uneventful recovery from surgery. During the second phase, four animals were excluded from group 1 and two from group 2. The exclusion was due to graft thrombosis and abscess (n = 4 for group 1, n = 2 for group 2), and narrowed/malformed utero-uterine anastomosis (additionally for n = 1, group 1) on examination at relaparotomy (Table 2). Relaparotomy (along the scar of the original laparotomy) was performed for all females 2 weeks post transplantation, as the physical appearance of the animals had little value as an indicator of graft health. Overall, the 2 week graft survival rate was 50% and 75% for groups 1 and 2, respectively (Table 3).
During phase 3, four females from group 1 were matched for mating with Lewis males, around 9 weeks after UTx. Two females showed signs of pregnancy (bodyweight increase, Figure 3; nesting behavior); however, no live birth was observed. After two mating cycles of three females, pup body parts (bone and tissue) were found in one female rat (°1). Histological examination of hematoxylin and eosin stained tissue sections by a veterinary pathologist revealed these pups developed up to parturition (Figures 4 and Figure 5).
Six females from group 2 were mated with Lewis males (see Figure 6 for bodyweight changes). Three of the six rats (two Lewis and one Brown Norway rat) gave birth to pups, while another two showed signs of pregnancy. The first litter of the female Lewis rat (#1) consisted of two pups (Figure 7). Shortly after birth, the Lewis female became pregnant again; however, only two of three pups survived postnatally (Figure 8). One likely explanation for the one death is infanticide, as it occurs even with healthy pups under conditions of postpartum stress. Likewise, the Brown Norway female (#2) gave birth twice, each time to four pups per mating cycle (Figure 9). The largest litter number of group 2 was delivered by another Lewis female (#3), with seven pups after the first mating cycle. All surviving pups displayed normal development (Figure 10).
Overall, the adaptation of the protocol increased 2 week graft survival from 50% to 75%. Five of six females became pregnant, compared to two out of four from group 1. Likewise, three of six of females gave birth to live pups compared to zero out of four of the group 1 females. In conclusion, the adapted protocol improved both direct surgical outcomes and the rate of successful live births following UTx (Table 4 and Figure 6).
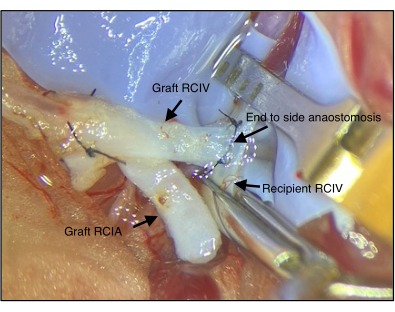
Figure 1: Anastomosis of the graft and the recipient's vein. The right common iliac vein (RCIV) of the graft is connected to the RCIV of the recipient via end-to-side anastomosis (step 2.4). RCIA = right common iliac artery Please click here to view a larger version of this figure.
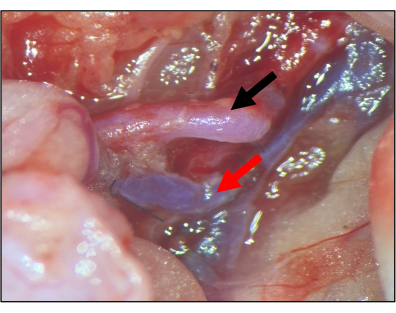
Figure 2: Anastomosis of the graft and the recipient artery. The right common iliac artery (RCIA) is connected to the RCIA of the recipient via end-to-side anastomosis (step 2.4). After opening both vascular clamps (2.5), the artery should be fully perfused in the absence of outer bleeding. Black arrow: graft RCIA; red arrow: graft RCIV. Please click here to view a larger version of this figure.
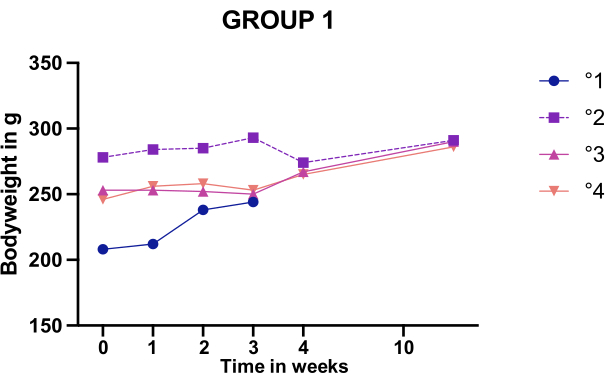
Figure 3: Bodyweight changes after mating of females in group 1. Body weight monitoring of the four group 1 females who displayed an intact graft upon relaparotomy. One animal (°1) was euthanized during Caesarean sectioning to inspect the uterus. Please click here to view a larger version of this figure.
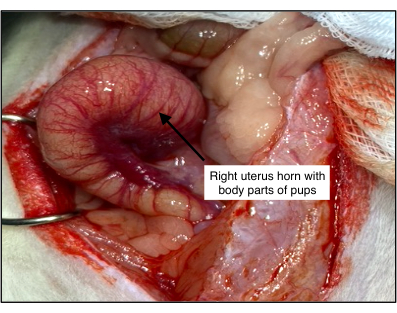
Figure 4: Histological examination of the uterus of the group 1 rat with dead pups. Body parts of pups were found in rat °1. Examination revealed a vital and dilated uterus, suggesting the pups developed normally but could not be delivered. Please click here to view a larger version of this figure.
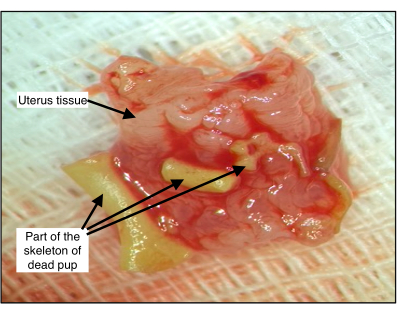
Figure 5: Pup body parts inside the uterus of group 1 rat °1. The developmental stage of the bones was consistent with full-term pups. Please click here to view a larger version of this figure.
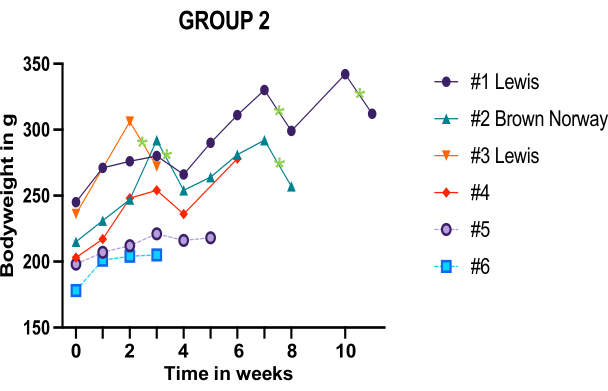
Figure 6: Body weight monitoring of the six group 2 females who displayed an intact graft upon relaparotomy. Green stars mark individual birth events. Hashtag numbers refer to the individual females. Please click here to view a larger version of this figure.

Figure 7: The first live birth after rat UTx following the modified protocol. Two newborn rats and their mother (head to the right; Lewis female #1, group 2). Please click here to view a larger version of this figure.

Figure 8: The second litter after the second mating cycle post rat UTx following the modified protocol. Female #1 (group 2) gave birth to three pups, two of which survived. Please click here to view a larger version of this figure.

Figure 9: The first litter of the Brown Norway rat after UTx following the modified protocol. After the first mating cycle, the Brown Norway rat (#2, group 2) gave birth to four pups, followed by another four after the second mating cycle. Please click here to view a larger version of this figure.
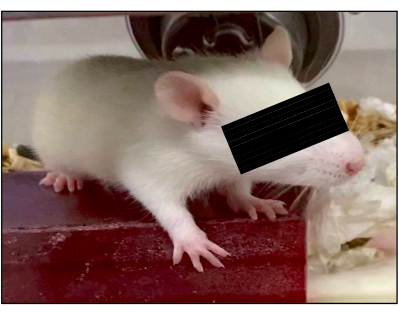
Figure 10: Development of pups. All surviving pups displayed normal development at 3 weeks of age. One representative example is shown. Please click here to view a larger version of this figure.
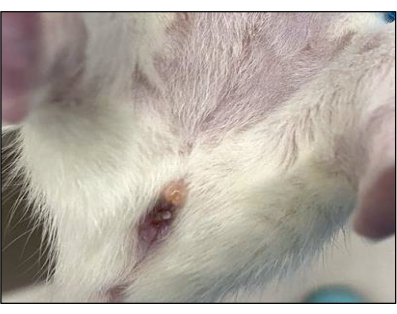
Figure 11: Vaginal plug formation following successful mating. White plugs should form to cover the vagina after fertilization to prevent further mating. Please click here to view a larger version of this figure.
| Group 1 | Group 2 | Syngeneic UTx in rats | Allogeneic UTx in rats | |
| before modification | after modification | see ref. 12 | see ref. 15 | |
| Total number of animals | 8 | 8 | 27 | 14 |
| Two-weeks graft survival | 4/8 (50%) | 6/8 (75%) | 19/27 (70%) | 9/14 (64%) |
| Number of mated females | 4/4 (100%) | 6/6 (100%) | 17/19 (89%) | 9/9 (100%) |
| Full term pregnancy | 1/4 (25%) | 5/6 (83%) | 11/17(65%) | 5/9 (56%) |
| Successfully delivered litter | 0 | 5a/td> | 1 | 5 |
| Total number of living pups | 0 | 20b | 3c | 25d |
| Pregnancy to term w/o live birth | 1 | 1e | 10 | 2 |
Table 1: Outcome comparison of the modified and unmodified protocol for rat UTx. a: Two pregnancies by the same rat; b: Including the infanticide pup; c: Median; d: Sum of the median/delivery; e: Dead pups in resorption stage after three cycles of mating.
| Surgical settings | Group 1 (n = 8) | Group 2 (n = 8) |
| Project stage | initial stage | late stage |
| Cold storage time | 2-3 h | 2-3 h |
| Flushing solution during anastomosis | RH | RHX |
| Vaginal anastomosis | 6/0 Ethilon | 6/0 Vicryl |
| Uterus horn anastomosis | partially continuous suture | interrupted suture |
| Arteria anastomosis | continuous suture | Interrupted and continuous |
| Micro-vascularization around vagina and cervix | cauterization close to the vaginal/cervical tissue | cauterization more distally |
Table 2: Surgical settings group 1 versus group 2.
| Exclusion criteria# |
| Signs of thrombosis (particularly around anastomoses) |
| Major adhesion |
| Constricted uterus |
| Signs of infection |
| Graft necrosis |
Table 3: Exclusion criteria for mating. #Applied at relaparotomy 2 weeks post UTx.
| n (group 1) | n (group 2) | |
| Animals | 8 | 8 |
| Healthy graft after 2 weeks | 4 | 6 |
| Mated | 4 | 6 |
| Full term pregnancy | 1 | 5 |
| Successfully delivered litter | 0 | 5a |
| Total number of living pups | 0 | 20b |
| Pregnancy to term, not live birth | 1 | 0 |
Table 4: Outcomes of group 1 versus group 2. a: Two consecutive pregnancies in the same rat; b: Including the pup killed by infanticide.
