MSC-encapsulated HA hydrogels were cultured in chondrogenic medium supplemented with TGFβ3, an inducer of chondrogenesis41 (step 4.1). We compared the properties of HA with those of collagen, which has been shown to be effective in creating MSC-based artificial cartilage grafts for endochondral ossification, as described previously38. Undifferentiated MSCs were not included as negative controls in this study because it has been demonstrated that undifferentiated MSCs require mineralized surfaces as a priming substrate to generate bone by osteogenic differentiation (i.e., intramembrane ossification)7.
The size of the hyaluronan hydrogels did not change throughout the in vitro culture period, as judged based on diameters measured under an inverted microscope, whereas the collagen hydrogels used for comparison began to shrink soon after the culture started. To reduce the size difference between the HA and collagen constructs after in vitro culture, the number of MSCs and the volume of the gel used to create the HA hydrogels were halved compared to those used for the collagen hydrogels. However, the wet weight of the HA constructs after 3 weeks of cartilage culture was 4x heavier than that of the collagen constructs.
Chondrogenic and hypertrophic differentiation in vitro.
After chondrogenic differentiation (at week 3 of in vitro culture), sulfated glycosaminoglycans (sGAG)-positive (Safranin O/fast green staining; Figure 3A) and type II collagen-positive extracellular matrix was observed in both constructs, indicating that both HA and collagen hydrogels supported chondrogenesis. However, compared to the collagen construct, the distribution of sGAG, type II collagen (Col II), and type X collagen (Col X) were more homogeneous throughout the tissue in the HA constructs. Differences between the two constructs were also apparent in cell morphology: cells with a chondrocyte-like rounded morphology were distributed throughout the tissue in the HA constructs. In the collagen constructs, however, cells in the periphery showed a heterogeneous morphology, ranging from irregular/stretched to rounded morphology. Consistent with this, the average roundness of cells in the HA constructs was higher than in the collagen constructs, both in the periphery and central regions (34% versus. 77.6% (p<0.01) and 78.3% vs. 100% (p<0.05), respectively; Figure 3B). At 5 weeks of culture, calcium deposition was detected at the outer edges in both constructs (alizarin red; Figure 3C). Furthermore, expression of chondrogenic (Sox-9, aggrecan (ACAN), Col II), hypertrophic (Col X, matrix metallopeptidase 13 (MMP-13)), and osteogenic (type I collagen (Col I), bone sialoprotein (BSP), osteocalcin (OCN)) markers14 was detected by quantitative real-time RT-PCR, confirming the progression of chondrogenic and hypertrophic differentiation during in vitro culture (Figure 4).
Endochondral ossification of subcutaneously implanted constructs in vivo.
Subcutaneous pockets were created on the back of nude mice, and two to three constructs were implanted in each pocket after hypertrophic differentiation (at week 5 of in vitro culture). At 4 or 8 weeks after implantation, all HA constructs were attached to each other in the implanted pockets (Table 1). In the collagen constructs, adhesion was observed in 60% of the pockets, while in the remaining pockets, the grafts were independent of each other. Hematoxylin and eosin (H&E) staining revealed that in both constructs at 8 weeks post-implantation, osteoid tissue with lamellar morphology was formed in the outer regions of the constructs (Figure 5Aa,f). sGAG staining disappeared in the HA constructs, indicating the loss of their cartilage phenotype (Figure 5Ah). In both constructs, a bone marrow component containing hematopoietic cells and adipose tissue was formed between the inner cartilage and the outer osteoid tissues. In all HA constructs, the bone tissues of the fused constructs were connected and surrounded by joint fibrous tissue and bone marrow developed along the space between the two adherent constructs, indicating that multiple HA constructs tend to form integrated bone tissue (Figure 5Ag). The adhered collagen constructs were similarly integrated in two of the three fused cases, but in the third case, the bone tissue of the two constructs was not connected (Table 1 and Figure 5Ab). In both constructs, vessels identified by CD31-positive endothelial cells42 were observed in the bone marrow (Figures 5Ad,i), and the inner cartilage regions were surrounded by TRAP-positive multinucleated cells of the osteoclast lineage, indicating that cartilage tissue was subject to remodeling (Figures 5Ae,j).
Mineral was deposited in the outer osteoid region in both HA and collagen constructs (Figure 5B). While the total mineral density of the new bone was similar between HA and collagen constructs, the mineral volume was significantly higher in the HA constructs than that in the collagen constructs, which may reflect the fact that HA hydrogels did not shrink during in vitro culture, resulting in larger constructs than collagen hydrogels (Figure 5C,D).
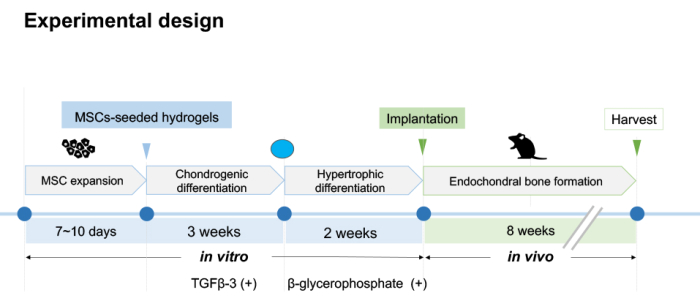
Figure 1: Experimental design. The first step of this protocol is to encapsulate expanded MSCs in HA hydrogels to promote chondrogenic and hypertrophic differentiation in vitro. Constructs are cultured in chondrogenic differentiation conditions for 3 weeks, followed by an additional 2 weeks in hypertrophic differentiation conditions. The second step of this protocol is to subcutaneously implant the constructs into nude mice at week 5 of in vitro culture to undergo endochondral ossification in vivo for 8 weeks. Please click here to view a larger version of this figure.
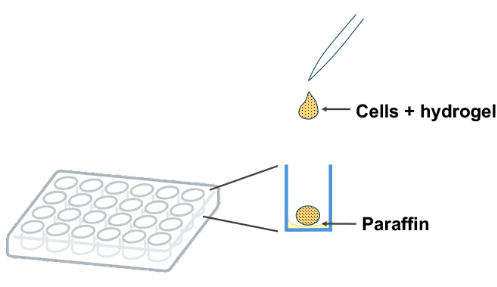
Figure 2: Preparation of MSCs-seeded hydrogels. Drop modified HA/crosslinker solution containing MSCs onto a paraffin-coated 24-well plate and allow to solidify at 37 °C for 30 min. Please click here to view a larger version of this figure.
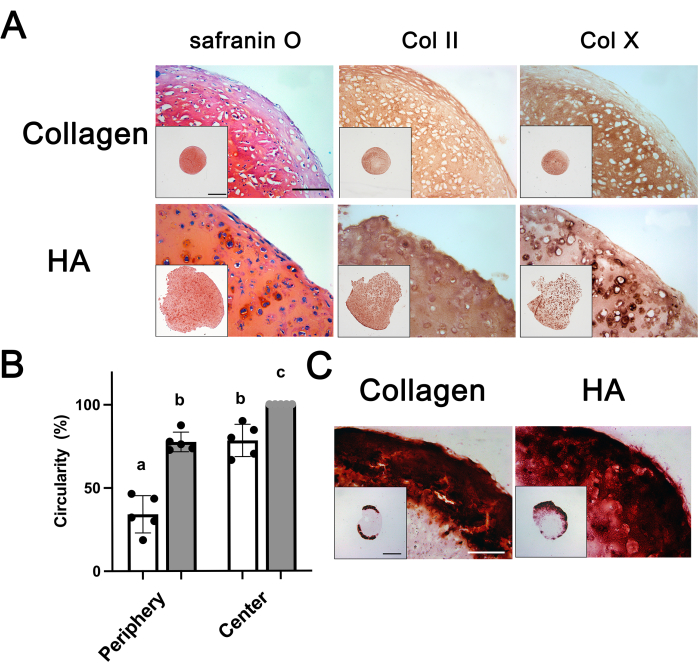
Figure 3: Histological and immunohistochemical analysis of HA and collagen constructs after in vitro culture22. (A) Constructs at 3 weeks (3W) of in vitro culture were stained for sGAG (safranin O/fast green), type II collagen (Col II), and type X collagen (Col X). (B) The average circularity values of cells at 3 weeks of in vitro culture (n = 5). Open and grey bars indicate collagen and HA constructs, respectively. Groups without a common letter are statistically different (a versus b, p<0.01; b versus c, p<0.05). (C) Constructs at 5 weeks (5W) of in vitro culture were stained for calcium (alizarin red). All pictures were captured with the same magnification (Scale bar: 200 µm). A low-magnification overview of the entire tissues is shown in the insets (Scale bar: 1 mm). Error bars represent mean ± standard deviation (SD). The one-way ANOVA followed by Tukey's multiple comparisons test was used to determine significant differences between groups. This figure has been modified from38. Please click here to view a larger version of this figure.
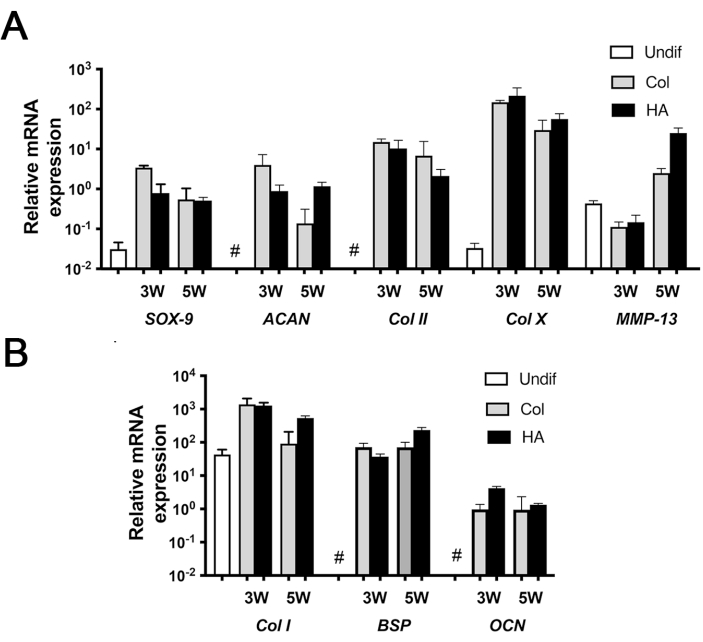
Figure 4: Gene expression analysis of HA and collagen constructs at 3 and 5 weeks of in vitro culture. (A) Chondrogenic and hypertrophic markers. (B) Osteogenic markers. Values are presented as mean ± standard deviation (SD) (n = 3). Undifferentiated MSCs expressed high levels of Col I and MMP-13 and low levels of Sox-9 and Col X; they did not express (#) ACAN, Col II, BSP, and OCN. Error bars represent mean ± standard deviation (SD). This figure has been modified from38. Please click here to view a larger version of this figure.
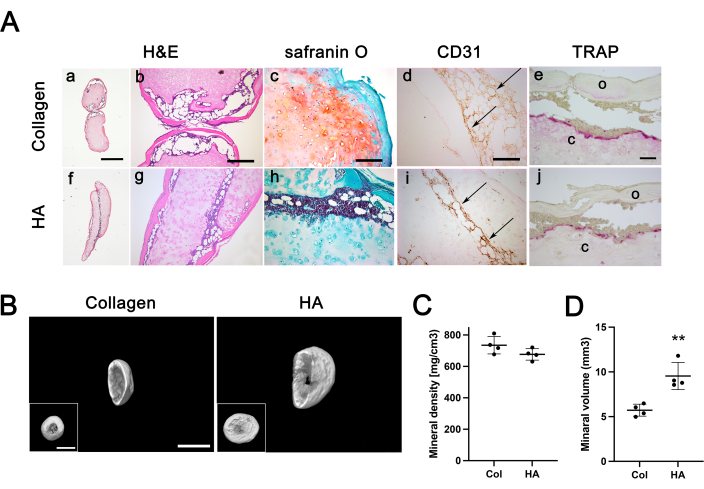
Figure 5: Immunohistochemical analysis and calcification of HA and collagen constructs post-implantation at 8 weeks. (A) Constructs were stained for Hematoxylin and Eosin (H&E, a, b, f, and g), safranin O/Fast Green (c and h), endothelial cells (Cluster of Differentiation 31, CD31) (d and i), and Tartrate-resistant acid phosphatase (TRAP, e and j). (a and f) Overview of the entire tissues (scale bar = 500 µm). H&E, safranin O, CD31: scale bar = 200 µm; TRAP: scale bar= 50 µm. Arrows indicate CD31-positive endothelial cells. Abbreviations: c = inner cartilage tissue; o = outer osteoid tissue. (B) MicroCT (µCT) imaging of collagen and HA constructs (main and inset image scale bars = 2 mm). (C,D) The total mineral density (C) and volume (D) of HA and collagen constructs (n = 4). ** indicates significant differences; p <0.01. Four constructs were analyzed per group using µCT. Error bars represent mean ± standard deviation (SD). Student's t-test was used to determine significant differences between groups. This figure has been modified from38. Please click here to view a larger version of this figure.
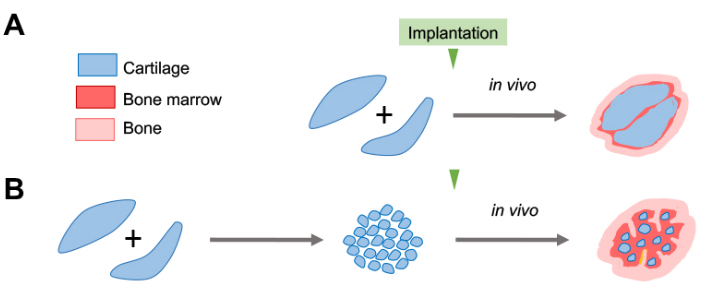
Figure 6: Strategy for facilitating ECOs using HA-based artificial cartilage. Schematic diagram of ossification and bone marrow development without and with fragmentation (µ-pellets) of implanted HA constructs. (A) HA hydrogels have an excellent fusion tendency to form an integrated bone with vascularization and marrow development between fused grafts in vivo. The resulting implanted tissue, however, remained predominantly in a cartilage state even 8 weeks post-implantation. (B) Given the tendency of HA constructs to fuse to form integrated bone, processing HA constructs into µ-pellets may accelerate the remodeling rate of transplanted tissue and promote bone formation. Micronizing the constructs increases surface area, which may promote the resorption of cartilage tissue and the formation of bone tissue and may also promote angiogenesis and bone marrow development because of the increased space for host cell infiltration. Please click here to view a larger version of this figure.
| Hydrogel | Experiments | Adhered | United | % United |
| Collagen | 5 | 3 | 2 | 40 |
| HA | 5 | 5 | 5 | 100 |
Table 1: Unification rate when multiple constructs were implanted in a single pocket. Two or three constructs were subcutaneously implanted in a single pocket. Constructs were harvested 4- or 8-weeks post-implantation and histologically examined.
