Robotic D3 Partial Duodenal Resection with Primary Side-to-Side Anastomosis
Summary
This protocol presents a case of a robotic partial duodenal resection with primary side-to-side duodeno-jejunal reconstruction in a patient with a 5 cm duodenal stenosis. This is done at the third duodenal segment (D3) after an endoscopic mucosal resection (EMR) for a duodenal polyp.
Abstract
Duodenal stenosis is a condition that can be related to several diseases, being either intrinsic, such as neoplasm and inflammatory stenosis, or extrinsic, such as pancreatic pseudocyst, superior mesenteric artery syndrome, and foreign bodies. Current treatments range from endoscopic approaches, such as endoscopic resection and stent placement, to surgical approaches, including duodenal resection, pancreaticoduodenectomy, and gastrointestinal bypass. Minimally invasive robot-assisted surgery is gaining importance due to its potential to decrease surgical stress, intraoperative blood loss, and postoperative pain, while its instruments and 3D-vision facilitate fine dissection and intra-abdominal suturing, all leading to a reduced time to functional recovery and shorter hospital stay. We present a case of a 75-year-old female who underwent robotic D3 partial duodenal resection with primary side-to-side duodeno-jejunal anastomosis for a 5 cm adenoma with focal high-grade dysplasia.
Introduction
Indications for partial duodenal resection are few and very specific. These mainly rely on treating gastrointestinal stromal tumors (GISTs), early duodenal carcinomas, and duodenal adenomas that cannot be removed endoscopically. Partial duodenal resection has gained relevance as an alternative to more invasive procedures such as pancreaticoduodenectomy. The anatomical complexity at the junction of the biliary tract, pancreas, and gastrointestinal tract, as well as the special physiological functions of the duodenum, makes it difficult for any surgeon to approach it during surgery. Therefore, as with any complex surgical technique, it is difficult to have a consensus of choice1,2. Due to its complexity and tight surgical indications, partial duodenal resection should be performed only at centers performing pancreatoduodenectomies.
In the last decades, there has been a rapid development in robot-assisted minimally invasive surgery with the aim to reduce pain and enhance recovery compared to open surgical procedures. Nowadays, when dealing with partial duodenal resection, reconstruction with Roux-en-Y anastomosis is feasible and reliable. Even if partial excision of the affected duodenum with side-to-side duodeno-jejunal anastomosis seems equally effective, technical difficulty and outcome of the methods have not been described in detail2,3.
We present a case of a 75-year-old female who underwent endoscopic mucosal resection (EMR) for a 5 cm adenoma with focal high-grade dysplasia, which results in reactive stenosis. Due to severe dysphagia, the inability to cure the stenosis with endoscopy, and the absence of relation to the papilla of Vater (no obstruction in the pancreatobiliary tree), the multidisciplinary team decided to enroll the patient in a robotic D3 partial duodenal resection with primary side-to-side duodeno-jejunal anastomosis.
Protocol
The present protocol follows the ethics guidelines of Amsterdam UMC. Informed consent was obtained from the patient for this article and the video.
1. Preoperative management
- Perform preoperative imaging with a CT scan to assess the localization and the extent of the duodenal stenosis and its relationship with the papilla of Vater (Figure 1).
- Perform esophagogastroduodenoscopy to describe the stenosis and its location. The duodenal lumen must be partially/entirely obstructed by the lesion, making it impossible for the endoscope to proceed any further and complete curative endoscopic treatment (Figure 2). Place, before the stenosis, a small 1 cm mark with an inked tattoo on the submucosa for intraoperative identification of the lesion.
- Evaluate the eligibility for the surgical approach and relative contraindications (severe stenosis causing dysphagia, pain, malnutrition, feasibility of treating the disease endoscopically, duodenal stenosis far and distal from the papilla of Vater, no history of abdominal surgery, and in more general terms any benign, premalignant, malignant local entity in D3 duodenum which can be treated with a partial duodenectomy).
2. Anesthesia, positioning of the patient, and safety check procedures
- Induce the patient with general anesthesia with the help of an anesthesiologist.
- Place the patient in a French position. Lower the right arm alongside the patient on an arm board while placing the left arm in a 90° position. Tilt the table 20° to the left of the patient and in a 20° reverse Trendelenburg position.
- Perform the safety check procedures as required by the Institution (e.g., patient's name and surname, date of birth, type of surgery, prophylactic antibiotic therapy, etc.) and create a sterile area using chloride surgical solution and surgical drapes.
3. Pneumoperitoneum creation and trocars' placement
- Insert a Veress needle at Palmer's point, 2 cm below the left coastal margin following the mid-clavicular line, in order to create a pneumoperitoneum. Then insufflate to 10-12 mm CO2.
- After insufflation, mark the positions of the trocars and place them as shown in Figure 3 (4 robot trocars, 2 (12 mm) laparoscopic table-side surgeon trocars).
- First, draw a line from a point, 2 cm to the right of the umbilicus to the costal margin left of the gallbladder. On this line, 11-12 cm downwards from the costal margin, mark the robotic camera trocar, number 3.
- At 7 cm distance left and right from trocar 3, mark trocars 2 and 4.
- Mark trocar 1, 7 cm craniolateral from trocar 2.
NOTE: This follows the Pittsburgh approach for robot-assisted pancreaticoduodenectomy4,5,6. However, this procedure can also be performed with only one laparoscopic trocar, which can later be used for the extraction of the specimen.
4. Port placement
- Insufflate with a Verres needle at the Palmers' point connected to the CO2 resource. Place a 12 mm table-side surgeon trocar, 7 cm from both robot trocars 2 and 3, to the right of the umbilicus.
- Place the four 8 mm robotic trocars as marked after inspection and removal of the Veress needle.
- Place a second 12 mm table-side surgeon trocar, 7 cm from both trocars 3 and 4.
NOTE: Make sure the distance between all the trocars is approximately 7 cm.
5. Docking
- Install the robot over the patient's right shoulder and dock the robot arms to the robotic trocars.
NOTE: The final operative setting is shown in Figure 3 and Figure 4. To facilitate a large standalone 3D screen to the patient's right, have the robot come in cranially, over the patient's shoulder. To facilitate a comfortable position for the table-side surgeon, ensure that this surgeon sits down with cranially placed trocars and a favorable screen position.
6. Treitz mobilization
- Cranialize the greater omentum and colon by pushing them aside towards the diaphragm.
- Identify the first jejunal loop from the retroperitoneal cavity through the Treitz ligament.
- Dissect the left side of the ligament of Treitz to free the most distal part of the duodenum and the first part of the jejunum from the aorta using the robotic cautery hook on arm 4 and the laparoscopic vessel sealer.
7. Ascending colon and hepatic flexure mobilization
- Perform tunneling through the hepatocolic ligament in order to spare vascular structures.
- Perform mobilization of the hepatic flexure and the ascending colon using the robotic cautery hook on arm 4 and the laparoscopic sealing device.
NOTE: Pay attention to any vascular abnormalities of the right colonic artery.
8. Pancreatic head identification and mobilization
- Perform the Kocher maneuver by mobilizing the duodenum and the head of the pancreas from the caudal to cranial using the robotic cautery hook and the laparoscopic sealing device. To do so, incise the peritoneum at the right edge of the duodenum and move the duodenum and the head of the pancreas to the left of the patient7.
- Perform the traction of the jejunal loop in the retroperitoneal cavity.
9. Duodenal resection
- Staple the intestinal loop, 10 cm distally, to the submucosal tattoo.
- Detach the duodenum from its mesentery using a laparoscopic sealing device, by performing a safe and feasible dissection of the mesentery.
- Staple the duodenum at the level of the submucosal tattoo, including the tattoo in the specimen. A robotic endo stapler can be used as well.
NOTE: The minimum distance of the lesion from the papilla of Vater should be 5 cm. In other situations (e.g., 2-5 cm), a Fogarty balloon-tipped catheter can be passed through the papilla of Vater. This can be confirmed intraoperatively by endoscopy.
10. Duodeno-jejunostomy
- Create two small enterotomies using robotic scissors with diathermia at the antimesenteric side of the duodenal and jejunal stump.
- Make a side-to-side jejuno-jejunostomy of 60 mm using an endo-stapler with a vascular cartridge (white cartridge).
- Close the remaining anastomosis opening with two layers of running 4-0 suture (~15 cm).
11. Drain-placement
- In case of a misfire of the stapler or in case of accidental contamination of the abdomen from intestinal fluids, place a drain.
NOTE: Drain was not placed in this specific case. The patient underwent elective operation with no operative events, so no drain was needed.
12. Postoperative management
- Remove the nasogastric tube early in the morning of postoperative day 1. Start a soft liquid diet and move on to a normal diet in 24 h.
- Assess serum C-reactive protein (CRP) and leucocyte levels on postoperative days 2, 3, and 4. Perform a CT or MRI scan of the abdomen if CRP on day four is elevated compared to day three or when there are undesired changes in the postoperative course (drain quality, insufficient clinical improvement).
- Discharge the patient earlier if clinically well, eating sufficiently, pain-free, and CRP <150.
NOTE: The patient was discharged on postoperative day 3, almost pain-free, clinically well, with a CRP value of 67 mg/L.
13. Post-discharge management
- Perform follow-up medical examination after 10-14 days.
Representative Results
Representative results are shown in Table 1. The operative time was 84 min with 20 mL of blood loss. The postoperative course of the patient was uneventful. The nasogastric tube (NGT) was removed early in the morning of postoperative day 1 (POD1). The patient restarted feeding at POD2 and was discharged in a good condition on POD3. Pathological assessment reported the removal of a 5 cm adenoma with focal high-grade dysplasia and negative margins.
The patient had a follow-up visit two weeks after surgery, where she reported postprandial pain associated with episodes of vomit and occasional episodes of fever (T°< 38 °C). She underwent a CT scan, which reported no fluid collection in the abdomen and no signs of suffering to the liver, pancreas, stomach, and small intestine (Figure 5 and Figure 6). At a further follow-up visit, the patient reported a total reduction of the previously reported symptoms. The surgical follow-up was then stopped.
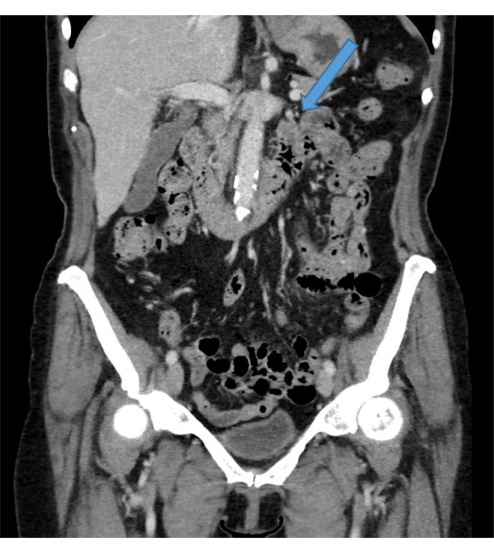
Figure 1: Preoperative assessment. Preoperative imaging with CT scan to assess the localization and the extent of the duodenal stenosis. Please click here to view a larger version of this figure.

Figure 2: Preoperative assessment. Preoperative gastroscopy to describe the stenosis, its location, and its relationship with the papilla of Vater. Please click here to view a larger version of this figure.
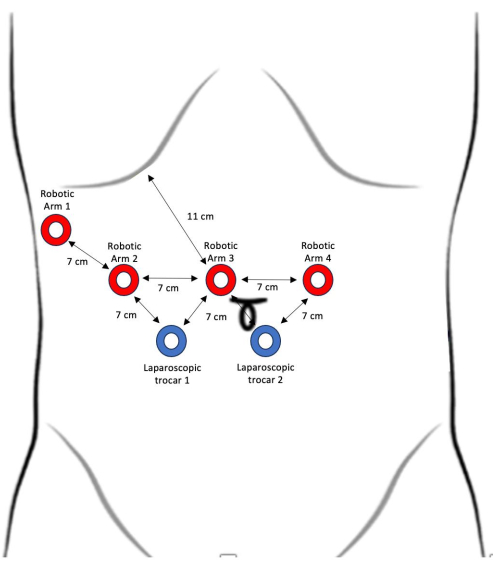
Figure 3: Trocars' placement. Red: 8 mm robotic trocars, blue: 12 mm laparoscopic trocars, yellow: 5 mm trocar for stomach/liver retractor. Please click here to view a larger version of this figure.
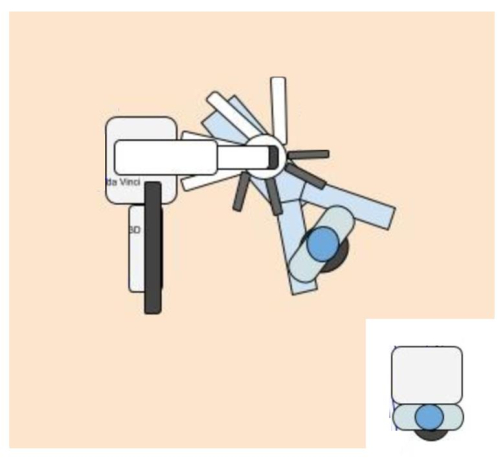
Figure 4: Set up of the robot during surgery. Please click here to view a larger version of this figure.

Figure 5: Coronal plane CT scan performed two weeks after surgery. Coronal plane at the level of the duodeno-jejunal anastomosis Please click here to view a larger version of this figure.

Figure 6: Axial plane CT scan performed two weeks after surgery. Axial plane at the level of the duodenojejunal anastomosis Please click here to view a larger version of this figure.
| Intraoperative | |
| Operative time, minutes | 84 |
| Intraoperative blood loss, ml | 20 |
| Postoperative | |
| Postoperative complications | none |
| Hospital length of stay, days | 4 |
| Discharge, postoperative day | 3 |
| Pathology | Radical removal of a 5cm adenoma High-grade dysplasia |
Table 1: Representative results of the surgery.
Discussion
Stenosis of the duodenum produces vague and confounding symptoms whose severity is mainly related to its severity (partial stenosis, total obstruction) and is often resistant to early attempts at diagnosis. Given the underlying anatomical complexities, the choice of treatment options is difficult, and if possible, it should only be undertaken by an adequate multidisciplinary team (MDT)3,8,9 with experience in robotic pancreatoduodenectomy10,11.
Performing a proper preoperative investigation is crucial. Indeed, endoscopic procedures, such as enteroscopy and endoscopic ultrasound (EUS), are mandatory for investigating the extension of stenosis and its relationship to the papilla of Vater. During the endoscopic procedure, marking with a small 1 cm submucosal ink tattoo, proximally to the lesion, supports intraoperative identification and obtaining negative surgical margins.
The real advantage of limited resection is the possibility of avoiding invasive procedure, such as pancreaticoduodenectomy (PD), without increasing the postoperative morbidity and decreasing the long-term survival12. Due to this rationale, minimally-invasive surgery should be taken into consideration. Indeed, both laparoscopic and robotic approaches could be used to perform this type of intestinal resection. However, the robotic approach has several benefits compared to the laparoscopic approach. Indeed, high-definition 3D vision facilitates and magnifies instrument movement, whereas wristed instruments allow easier intra-abdominal suturing as compared to laparoscopy.
In 2021, a single-center retrospective study in patients with duodenal gastrointestinal stroma cell tumors reported benefits of the robotic approach, compared to the open approach, in terms of a shorter operative time, less intraoperative bleeding, and smaller surgical incisions2. Partial excision of the affected duodenum with side-to-side duodeno-jejunal anastomosis remains controversial due to the technical difficulty of this procedure2,3, particularly concerning the anastomosis. Indeed, a partial duodenectomy is mainly combined with a Roux-en-Y anastomosis since it is feasible and reliable. However, it should be taken into consideration that Roux-en-Y reconstruction could hold an increased risk of gastrointestinal leak due to the execution of one additional anastomosis compared to side-to-side duodeno-jejunal anastomosis.
As far as malignant diseases are concerned, the choice of the type of surgery is controversial. Some surgeons prefer pancreatoduodenectomy to reduce the risk of residual disease, even if it results in significantly higher postoperative morbidity and mortality13. Besides the higher perioperative morbidity and mortality rates, it is mandatory to consider that pancreatoduodenectomy is mainly performed when dealing with advanced diseases like carcinoma, which in itself has a high recurrence rate14. Recently, it has been reported that limited segmentectomy for limited duodenal cancer appears to offer statistically equivalent long-term survival rates with considerably less morbidity15. Additionally, specific preoperative factors such as tumor, node and metastasis (TNM) stage, tumor grade on histological report, and preoperative radiotherapy seem to be more reliable predictors of patient outcomes than the type of resection15.
A recent systematic review reported that in patients with cancer-related gastric outlet obstruction, endoscopic stent placement is associated with many positive outcomes compared to gastro-jejunostomy, including reduced hospital stays, lower postoperative mortality, and faster relief of symptoms, despite comparable benefits and complication rates16. However, in patients with longer prognoses, recurrence of obstructive symptoms appears to be significantly more likely after stent placement17. This scenario may encourage stronger consideration of surgical approaches to avoid the need for endoscopic re-intervention.
The main limitation of this surgical technique is related to identifying the diseased loop. Indeed, a small, inked tattoo is the only way to define where the lesion is and perform the resection. However, ink may spread too widely along the submucosa and mark the entire loop, making it almost impossible to identify the correct lines of resections. In order to reduce this risk, the ink tattoo must be as small as possible, and this should be communicated, prior to endoscopy, to the responsible gastroenterologist.
In conclusion, robotic partial duodenal resection with primary side-to-side duodeno-jejunal anastomosis is possible, especially if performed in patients with benign disease (e.g., inflammatory duodenal stenosis) and in highly specialized centers. Future larger prospective studies should confirm the safety and efficacy of this approach.
Declarações
The authors have nothing to disclose.
Acknowledgements
The clinical research was enabled by HPB-Amsterdam and F de Graaf, operating rooms Amsterdam UMC.
Materials
| SYSTEM | |||
| da Vinci Surgeon Console | IS | SS999 | Used to control the surgical robot. |
| da Vinci Vision Cart | IS | VS999 | The vision cart houses advanced vision and energy technologies and provides communications across da Vinci system components |
| da Vinci Xi | IS | K131861 | The surgical robot: ’patient side-cart’ |
| INSTRUMENTS | |||
| Cobra Liver Retractor Diamond-Flex | CareFusion | 89-6216 | Retracting the liver for optimal exposure of the surgical site. |
| da Vinci Xi Endoscope with Camera, 8 mm, 30° | IS | 470027 | The camera of the da Vinci robot. |
| ENDOEYE Rigid Video Laparoscope, 10 mm, 30° | Olympus | WA50042A | Toseewithintheintra-abdominal cavity. |
| ENDOWRIST Fenestrated Bipolar Forceps | IS | 470205 | Used for dissection and coagulation |
| ENDOWRIST HOT SHEARS | IS | 470179 | Used for cutting and coagulation. |
| ENDOWRIST Mega SutureCut Needle Driver | IS | 470309 | Used as a needle driver. |
| ENDOWRIST Permanent Cautery Hook | IS | 470183 | Used for coagulation. |
| ENDOWRIST PROGrasp Forceps | IS | 470093 | Used for dissection. |
| LigaSure Maryland Jaw | Medtronic | LF1937 | Used for vessel sealing |
| SUTURES | |||
| Vicryl 2-0 x2 | |||
| V-loc barbed 4-0 15 cm x2 | |||
| Monocryl 4-0 x2 | |||
| STAPLER | |||
| Echelon 60mm white cartridge | Ethicon | GST60W | Used for stapling |
Referências
- Lee, S. Y., et al. Surgical strategy and outcomes in duodenal gastrointestinal stromal tumor. Annals of Surgical Oncology. 24 (1), 202-210 (2017).
- Zhou, Z. -. P., et al. Robotic resection of duodenal gastrointestinal stromal tumour: Preliminary experience from a single centre. World Journal of Gastrointestinal Oncology. 13 (7), 706-715 (2021).
- McGuirk, M., Gachabayov, M., Gogna, S., Da Dong, X. Robotic duodenal (D3) resection with Roux-en-Y duodenojejunostomy reconstruction for large GIST tumor: Step by step with video. Surgical Oncology. 36, 130 (2021).
- Nota, C. L., et al. Developing a robotic pancreas program: the Dutch experience. Journal of Visualized Surgery. 3, 106 (2017).
- Hogg, M. E., et al. Mastery-based virtual reality robotic simulation curriculum: the first step toward operative robotic proficiency. Journal of Surgical Education. 74 (3), 477-485 (2017).
- Tam, V., et al. Robotic pancreatoduodenectomy biotissue curriculum has validity and improves technical performance for surgical oncology fellows. Journal of Surgical Education. 74 (6), 1057-1065 (2017).
- Niederle, B. V. . Surgery of the Biliary Tract. , (1981).
- Marano, A., et al. Robotic treatment for large duodenal gastrointestinal stromal tumor. Annals of Surgical Oncology. 27 (4), 1101-1102 (2020).
- Thomas, J., Abraham, K., Osilli, D., Mukherjee, S. Adult distal duodenal obstruction: a diagnostic and therapeutic challenge. Cureus. 14 (4), e24095 (2022).
- Emmen, A. M. L. H., et al. Impact of shifting from laparoscopic to robotic surgery during 600 minimally invasive pancreatic and liver resections. Surgical Endoscopy. 37 (4), 2659-2672 (2023).
- Zwart, M. J. W., et al. Outcomes of a multicenter training program in robotic pancreatoduodenectomy (LAELAPS-3). Annals of Surgery. 276 (6), e886-e895 (2022).
- Chok, A. -. Y., Koh, Y. -. X., Ow, M. Y. L., Allen, J. C., Goh, B. K. P. A systematic review and meta-analysis comparing pancreaticoduodenectomy versus limited resection for duodenal gastrointestinal stromal tumors. Annals of Surgical Oncology. 21 (11), 3429-3438 (2014).
- Lau, J. Y., et al. Through-the-scope balloon dilation for pyloric stenosis: long-term results. Gastrointestinal Endoscopy. 43 (2 Pt 1), 98-101 (1996).
- Shen, Z., et al. Pancreaticoduodenectomy versus limited resection for duodenal gastrointestinal stromal tumors: a systematic review and meta-analysis. BMC Surgery. 19, 121 (2019).
- Cloyd, J. M., Norton, J. A., Visser, B. C., Poultsides, G. A. Does the extent of resection impact survival for duodenal adenocarcinoma? Analysis of 1,611 cases. Annals of Surgical Oncology. 22 (2), 573-580 (2015).
- Nagaraja, V., Eslick, G. D., Cox, M. R. Endoscopic stenting versus operative gastrojejunostomy for malignant gastric outlet obstruction-a systematic review and meta-analysis of randomized and non-randomized trials. Journal of Gastrointestinal Oncology. 5 (2), 92-98 (2014).
- Jeurnink, S. M., van Eijck, C. H. J., Steyerberg, E. W., Kuipers, E. J., Siersema, P. D. Stent versus gastrojejunostomy for the palliation of gastric outlet obstruction: a systematic review. BMC Gastroenterology. 7, 18 (2007).
