Selecting a fabrication method is pivotal to ensure reproducible assay performances in paper-based immunoassay devices. In our study, we explored various manufacturing processes and materials in the context of demonstrating a paper-based immunoassay. Our chosen method utilizes a wax printing system to create hydrophobic barriers within paper-based microfluidic devices. This approach stands out due to its simplicity, speed, and consistent results. Of note, it offers the advantage of avoiding the use of photoresist chemicals, which have the potential to interfere with protein adsorption and increase the hydrophobicity of cellulose paper. Furthermore, wax printing ensures consistent dimensions of fluidic channels, contributing to repeatable assay performance.
Following the formation of hydrophobic barriers, the necessary reagents for the immunoassay were applied to the cellulose paper surface. With electrostatic adsorption, PLL assisted in biomolecule immobilization by interacting with both the positive charge of amine functional groups and the negatively charged antibody. This step facilitates the modification and immobilization of antibodies and the application of label-antibody conjugates during the fabrication processes. Importantly, this step can be conducted in parallel. The assembly of the paper immunoassay devices (DEN-NS1-PAD, as shown in Figure 1A) is completed by stacking the modified paper onto an adhesive plastic backing card and laminating it with a plastic film.
The main purpose of this study is to develop a user-friendly method utilizing a smartphone to measure NS1 concentrations. This approach could be used as a point-of-care testing (POCT) device in both home and clinical settings. Given the wide range of NS1 concentrations in patient serum, simple linear models were employed based on the results of these experiments. For each NS1 concentration, a dataset comprising three test devices was prepared. Photos of the devices were captured using a smartphone under standard settings and optimal lighting conditions, eliminating the need for a dark box. The test zone of the PADs contains mouse dengue NS1 monoclonal antibody, while the control zone features goat anti-mouse IgG antibody. With a sandwich assay format, higher NS1 concentrations in samples correspond to increased intensity of red color in the test zone. In contrast, the color intensity in the control zone remains relatively constant. Figure 1B showcases unprocessed smartphone images, which provide an advantageous visual observation without requiring specialized equipment.
Using a dedicated mobile application, we normalized the intensities and computed simple linear models for spiked NS1 concentrations in serum samples-the coefficient correlation (r2) obtained from the mobile application. The coefficient correlation (r2) obtained from the mobile application was 0.92 (Figure 3), aligning with expectations. This smartphone-based approach outperformed naked-eye observation, significantly enhancing sensitivity by 178%. Additionally, the limit of blank (LoB), limit of detection (LoD), and limit of quantification (LoQ) were calculated for the normalized intensities, as presented in Table 1.
Real-world clinical samples were utilized to demonstrate the practical functionality of DEN-NS1-PADs in clinical settings. The paper-based immunoassay produced qualitative color readouts within 20-30 min, allowing visual determination of negative or positive outcomes. Serum samples from patients suspected of dengue were subjected to the device. Figure 4 illustrates and compares the results obtained from both the device and a commercial rapid diagnostic test (RDT). Table 2 summarizes the outcomes of visual readings and the smartphone-based system. The commercial RDT and the device yielded similar results, with seven positive and 23 negative outcomes from visual reading. In contrast, the smartphone-based reader system exclusively applied to the device reported nine positive and 21 negative outcomes from clinical samples.
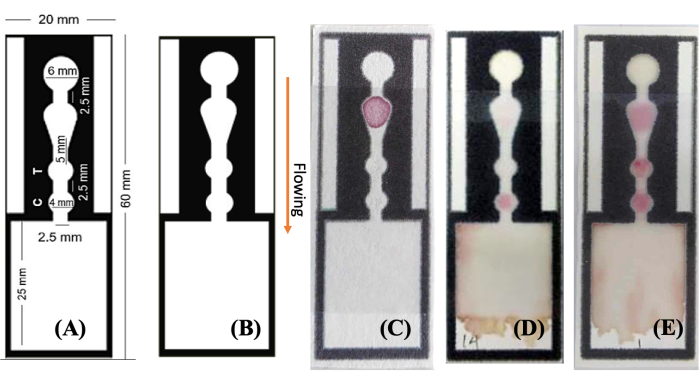
Figure 1: Images of designed and fabricated DEN-NS1-PAD. (A,B) A single channel from the wax-patterned hydrophobic barrier is designed and depicted in three states (C) before and (D,E) after introducing the sample solution to the designated area and showing the (D) negative and (E) positive results, respectively. The sample solution wicks through the channel (see arrow labeled), interacting with the components at key locations-AuNPs-Ab at the conjugate area, anti-NS1 antibody at the test area (indicative of a positive dengue NS1 result), and anti-mouse IgG at the control area. The results are readily observable by the naked eye and can be quantified by image processing using a flatbed scanner or smartphone camera. Abbreviation: AuNPs-Ab = gold nanoparticles-antibody conjugate. Please click here to view a larger version of this figure.
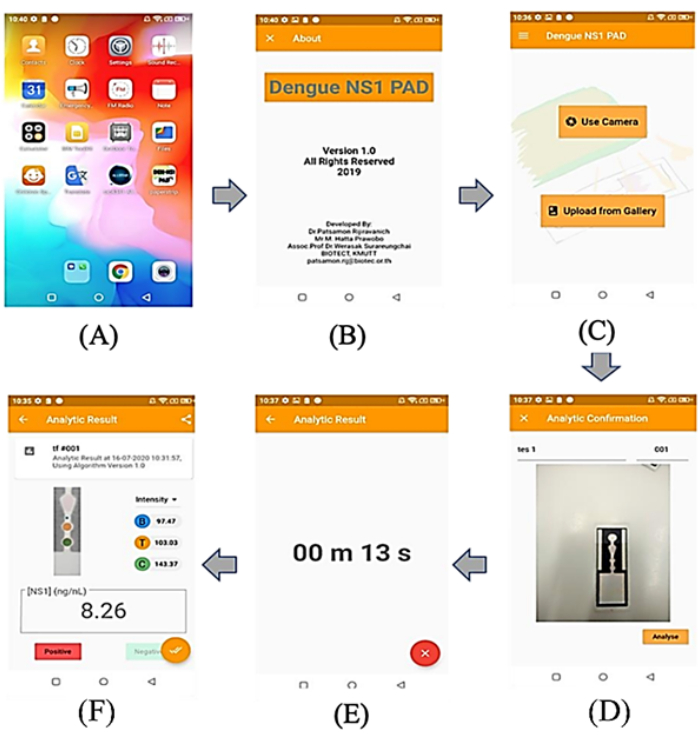
Figure 2: Screenshots of phone's screen from mobile app. (A) User screen of the Android application running on the mobile phone device, (B) display of application screen, (C) main menu of the application that the users can select to use camera or upload image from gallery, (D) display of a related image for testing, (E) display of the countdown time to analyze, (F) display of test results, including the intensity of the test and control zone, the decision of infection (positive/negative), and the concentration of NS1 in the sample. Please click here to view a larger version of this figure.
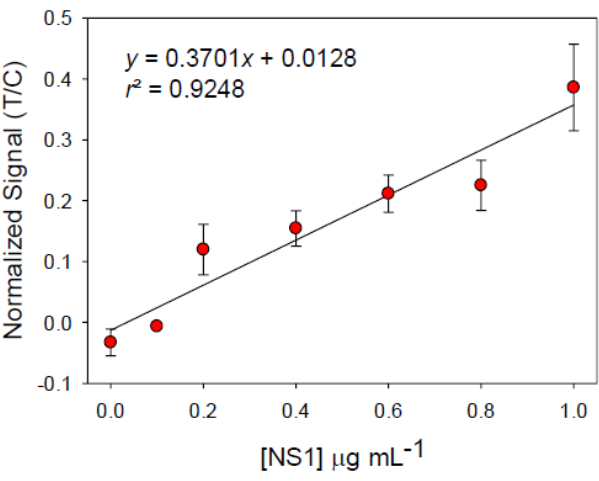
Figure 3: Linear calibration curve for NS1 detection in serum. The device was used and images interpreted by processing via an application based on smartphone data. The error bars show ±1 standard deviation, n = 3. Abbreviations: T = test area; C = control area. Please click here to view a larger version of this figure.
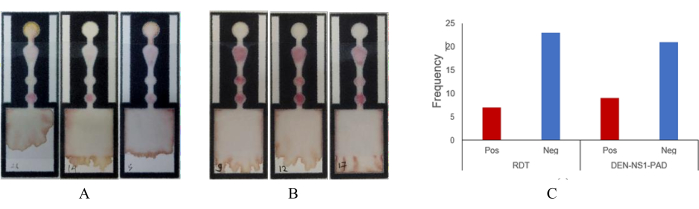
Figure 4: Image of DEN-NS1-PAD from the clinical sample assay. Serum (50 µL) was used in a paper-based immunoassay. (A) Negative result example, (B) positive results, (C) overall results and comparison of RDT versus paper-based immunoassay. Abbreviations: RDT = Rapid Diagnostic test; Pos = positive; Neg = negative. Please click here to view a larger version of this figure.
| Parameter | Naked eyes | Mobile App |
| Limit of Blank (LoB) | – | 43.15 ng mL-1 |
| Limit of Detection (LoD) | 200 ng mL-1 | 112.19 ng mL-1 |
| Limit of Quantification (LoQ) | – | 373.58 ng mL-1 |
Table 1: LoB, LoD, and LoQ from ImageJ and mobile application on data calibration standard NS1 in serum. Abbreviations: LoB = limit of blank; LoD = limit of detection; LoQ = limit of quantification.
| Patient No. | Naked Eyes | Smartphone App | ImageJ | |
| RDT | Paper-based Immunoassay | |||
| 1 | – | – | – | – |
| 2 | – | – | – | – |
| 3 | – | – | – | – |
| 4 | – | – | – | – |
| 5 | – | – | – | – |
| 6 | – | – | – | – |
| 7 | – | – | – | – |
| 8 | – | – | – | – |
| 9 | + | + | + | + |
| 10 | – | – | + | + |
| 11 | – | – | – | – |
| 12 | + | + | + | + |
| 13 | – | – | – | – |
| 14 | – | – | – | – |
| 15 | – | – | – | – |
| 16 | + | + | + | + |
| 17 | + | + | + | + |
| 18 | – | – | – | – |
| 19 | – | – | – | – |
| 20 | – | – | – | – |
| 21 | + | + | + | + |
| 22 | + | + | + | + |
| 23 | – | – | – | – |
| 24 | + | + | + | + |
| 25 | – | – | – | – |
| 26 | – | – | – | – |
| 27 | – | – | – | – |
| 28 | – | – | – | – |
| 29 | – | – | – | – |
| 30 | – | – | + | + |
Table 2: Comparison of visual reading and smartphone-based reader system results for serum samples. (+) and (-) indicate positive and negative interpretations of the results, respectively.
