The bioavailability of compounds delivered by topical administration to the surface of the eye is greatly limited, typically <5%1. Compounds administered by eye drops are mainly eliminated by drainage, induced lacrimation, tear fluid turnover, and conjunctival absorption. In addition, the permeation of compounds through the ocular surface is highly restricted by the cornea-conjunctiva barrier1,2,3. The cornea is composed of three main layers: the outermost epithelium, the intermediate stroma, and the innermost endothelium. The superficial corneal epithelium is interconnected by strong tight junctions and creates high paracellular resistance, which is the main barrier to substance permeability. Multiple epithelium layers further limit the permeation of hydrophilic and large molecules through the intercellular spaces of the cornea epithelium. Succeeding the epithelium, the stroma is composed of collagen fibers and contains aqueous pores. In contrast to the corneal epithelium, the stroma allows the movement of hydrophilic drugs; however, it is greatly impermeable to lipophilic compounds1,2,3. Together, the corneal epithelium and stromal layers present major tissue barriers that limit drug absorption. The corneal endothelium is not considered to restrict drug transport.
Alternative to the corneal delivery route is the conjunctival route. The conjunctiva is a multi-epithelium layer that covers the inner side of the eyelids and the anterior part of the sclera. The conjunctiva is characterized by fewer tight junctions than the corneal epithelium, allowing better permeability of hydrophilic drugs. However, vascularization of the conjunctiva results in systemic absorption of a large fraction of the administered molecules, again greatly limiting the bioavailability of delivered compounds to the anterior chamber1,2. An efficient way to bypass the outer ocular permeability barriers is to deliver the drug directly into the region of interest. For example, intravitreal injection is common for delivery into the vitreous humor4. Likewise, intracameral injection is utilized for delivery into the anterior chamber5. Establishing an efficient concentration at the anterior chamber is critical to various clinical situations, such as the treatment of infection by intracameral injection of antibiotics and postoperative anti-inflammatory treatments in cataract surgeries. Despite the advantage of improved substance bioavailability granted by intracameral injection, there are major safety concerns that should be considered. For example, intracameral drug injection may induce increased intraocular pressure, toxic anterior segment syndrome, and toxic endothelial cell destruction syndrome5,6. It is, therefore, essential to carefully assess in pre-clinical studies the efficacy and safety of drugs delivered by intracameral injections to maximize treatment efficiency and minimize potential adverse effects in patients.
Experimental animal models are indispensable in pre-clinical studies to investigate new treatments. Small rodents, such as mice and rats, are the most commonly utilized laboratory animals for such purposes. These animals exhibit numerous similarities to human anatomy and physiology, providing valuable insights. Moreover, their use is economically advantageous due to their small size, ease of maintenance, fast gestation, and ability to produce large numbers of offspring7.
Despite the widespread use of small rodents in eye disease models, their unique eye dimensions and anatomy pose significant challenges during experimental manipulations. For instance, procedures like intracameral injections, which are relatively straightforward in humans, become technically demanding in mice and rats. The challenges stem from factors such as the small volume of aqueous humor, the relatively large and inflexible lens, and the obstructive positioning and curvature of the lens within the rodents' eyes (Figure 1)8. These challenges increase the risk of damage during intracameral injections in rodents, leading to potential adverse effects and introducing experimental variability that can impact the validity of study conclusions. In our research, we have successfully developed a procedure for safe intracameral injection in rats. The technique involves creating a long, flat, self-sealing tunnel in the cornea into the anterior chamber. This method not only ensures precision but also enhances experimental reproducibility, addressing the issues associated with injection techniques in small rodents.
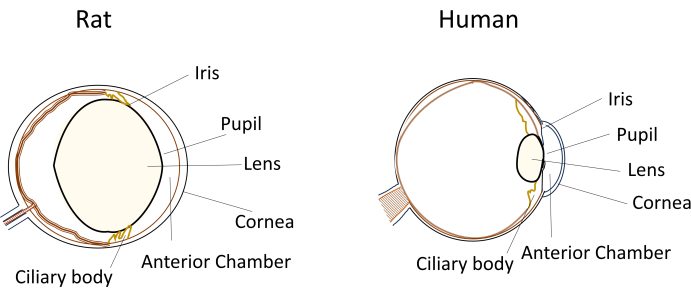
Figure 1: Schematic representation of the anatomical anterior segment features of rat and human eyes. Please click here to view a larger version of this figure.
The experiments in the protocol were approved by the National Permit Committee – for animal science and comply with the ARVO Statement the use of animals in ophthalmic and vision research. Female Sprague-Dawley rats, aged 8-10 weeks, were used for the present study and were exposed to 12/12 h light-dark cycles. The animals were obtained from a commercial source (see Table of Materials).
1. Animal preparation
- Prepare an anesthetic mixture of ketamine (80 mg/kg body weight in 0.8 mL) and xylazine (4 mg/kg body weight in 0.2 mL) and inject it intraperitoneally in a single injection to anesthetize the mice.
- Inject analgesic buprenorphine (0.03 mg/kg) intraperitoneally in a single injection.
- Apply topical ophthalmic anesthetic 0.4% oxybuprocaine to both eyes.
2. Creating a self-sealing corneal tunnel
- Stabilize the eye by holding the superior sclera at the vertical midline next to the corneoscleral junction with surgical ophthalmic forceps.
- Under a surgical microscope, place a sterile 0.8 mm, 31 G stiletto blade in the paracentral corneal region in the vertical midline (above the center of the pupil) in a flat position at an angle as close as possible to horizontal (Figure 2).
- In this position, puncture the cornea to make an incision and create a long tunnel (2-3 mm) until it penetrates into the central area of the anterior chamber. Avoid touching the lens (Figure 2).
NOTE: A successful tunnel will not induce leakage of the aqueous humor and shallowing of the anterior chamber. - Apply topical 0.3% ofloxacin and 0.1% dexamethasone to the injected eye.
- Examine under slit microscopy as follows.
- Observe the depth of the anterior chamber of the injected eye compared to the non-injected eye.
NOTE: The depth should be similar. - Observe the lens of the injected eye compared to the non-injected eye.
NOTE: The lens should be clear. Opacity may reflect lens damage during the surgical procedure.
- Observe the depth of the anterior chamber of the injected eye compared to the non-injected eye.
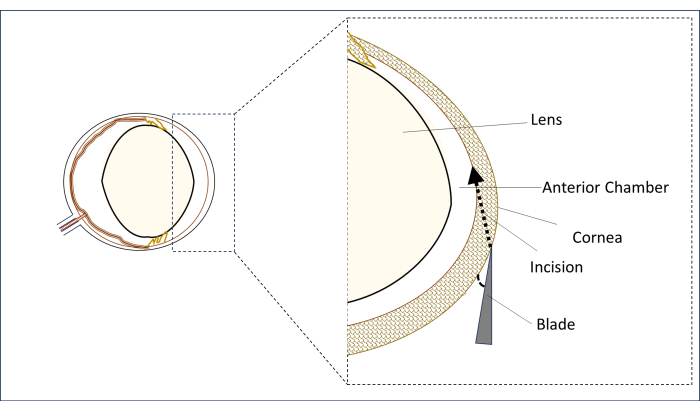
Figure 2: Schematic representation of the blade and incision angle and position. Please click here to view a larger version of this figure.
3. Option 1: Intracameral injection of trypan blue for assessing the successful injection into the anterior chamber
- Load 5 µL of trypan blue into a sterile 10 µL glass Hamilton syringe with a 34 G blunt needle.
NOTE: Injection of trypan blue is described as a means to evaluate the success of injection during the model calibration or setup stages. In the experimental settings, the syringe may be loaded with a solution of the compound of choice. - Insert the loaded syringe needle through the tunnel created in section 2 into the anterior chamber.
- Inject and hold the needle in place after injection for 2-3 seconds until all fluid clears.
- Remove the needle by pulling it out gently and slowly to avoid leakage from the corneal tunnel.
- Examine under slit microscopy. Evaluate the depth of the anterior chamber to exclude shallowing and verify the presence of trypan blue in the anterior chamber.
- Repeat slit examination after 24 h, 48 h, and 72 h.
4. Option 2: Intracameral injection of Hoechst for assessing the bioavailability of injected material to the endothelial cell layer
- Load 5 µL of Hoechst into a sterile 10 µL glass Hamilton syringe with a 34 G blunt needle.
NOTE: Injection of Hoechst is described as a means to evaluate the bioavailability of injected material by uptake into the endothelial cell layer and is useful during the model calibration or setup stages. In the experimental settings, the syringe may be loaded with a solution of the compound of choice. - Insert the loaded syringe needle through the tunnel created in section 2 into the anterior chamber.
- Inject and hold the needle in place after injection for 2-3 seconds until all fluid clears.
- Remove the needle by pulling it out gently and slowly to avoid leakage from the corneal tunnel incision.
- Approximately 15-20 min post-injection, euthanize the rats by intraperitoneal injection of 500 mg/kg sodium pentobarbitone.
- Enucleate both eyes and isolate corneas. Collect the non-injected cornea as a control.
- Stain both corneas with 0.5% Alizarin Red S according to manufacturer instructions to identify endothelial cells.
- Examine under a light microscope to image the alizarin-red staining of endothelial cells and under a fluorescent microscope to observe Hoechst staining, compared to the non-injected cornea as control.
Sprague Dawley rats were intracamerally injected with 5 µL of trypan blue according to the protocol described above. Slit lamp examination immediately after injection demonstrated that the chamber was stained with trypan blue, indicating that the injected material reached the anterior chamber (Figure 3). Furthermore, the anterior chamber depth was intact, suggesting that the injection did not cause leakage of aqueous humor and shallowing of the chamber.
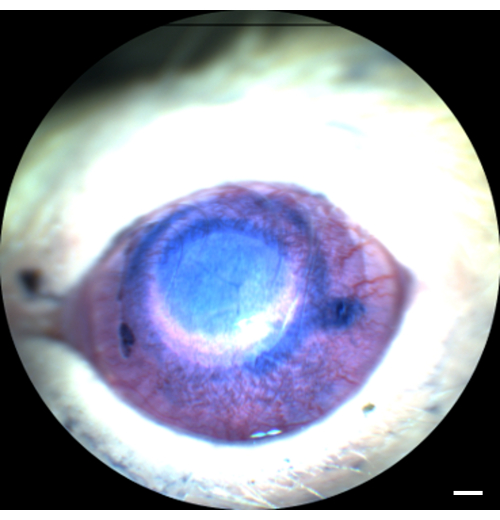
Figure 3: Intact anterior chamber following intracameral injection. Trypan blue was injected into the rat's anterior chamber. Slit microscopy examination demonstrates the presence of trypan blue without leakage or shallowing of the anterior chamber. Scale bar = 1 mm. Please click here to view a larger version of this figure.
Next, Hoechst, a cell-permeable fluorescent dye that binds DNA and stains cell nuclei, was injected to evaluate the bioavailability of drugs delivered by the described intracameral injection route. The uptake of Hoechst by endothelial cells was evaluated 15 min post-injection by isolating corneas and observing under a fluorescent microscope. To identify endothelial cells, the corneas were stained with Alizarin Red S, which stains the intercellular borders of the endothelium cell layer. As a control, we examined the non-injected eye from the same rat. Our results demonstrate that the endothelial cell layer was intact following injection, supporting that the described procedure does not cause damage to the endothelium. Furthermore, endothelial cells were positive for Hoechst nuclear staining, demonstrating the uptake of the injected Hoechst following intracameral injection (Figure 4).
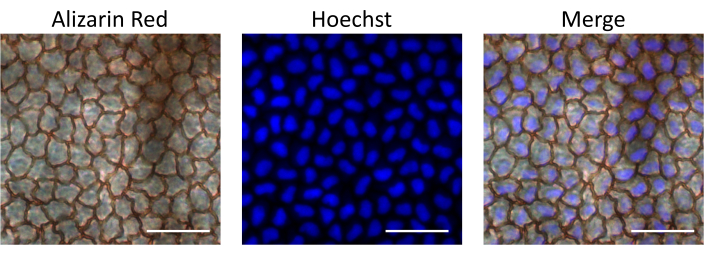
Figure 4: Bioavailability of intracamerally injected material to the endothelial cell layer. Hoechst was injected into the rat's anterior chamber. The cornea was isolated 15 min post-injection, stained with Alizarin Red S to observe endothelial cells, and imaged under a fluorescent microscope to observe Hoechst staining. Overlay images demonstrate nuclear Hoechst staining in corneal endothelial cells. Scale bars = 50 µM. Please click here to view a larger version of this figure.
