This study included 38 patients, all of whom completed the 2-week study (CG = 19, PG = 19). There were no significant differences in sex, age, surgical site, graft type, or degree of meniscus repair between the two groups (P > 0.05; see Table 1).
The intensity of pain of patients in EG on postoperative days 2, 7, and 14 was (2.2 ± 1.3), (1.1 ± 0.6), and (0.6 ± 0.5), respectively, indicating a gradual decrease in the intensity of pain. The intensity of pain was (2.5 ± 1.2), (1.5 ± 0.8), and (0.8 ± 0.5) in CG on postoperative days 2, 7, and 14, respectively, also indicating a gradual decrease in pain. DKE in both groups gradually decreased on postoperative days 2, 7, and 14 but there were no significant differences in pain intensity or DKE between the two groups (P > 0.05; see Table 2). All patients had good knee stability during rehabilitation, with good wound healing. None had positive anterior drawer tests, knee giving way, or falls.
AKROM in EG at 2, 7, and 14 days after surgery were (70.5 ± 17.0), (83.4 ± 13.5), and (98.1 ± 13.0), respectively, indicating gradual improvement in AKROM. AKROM in CG was (56.8 ± 13.1), (74.7 ± 12.9), and (87.0 ± 10.6), respectively, also indicating gradual improvement in AKROM. The ADL in EG on postoperative days 2, 7, and 14 were (72.8 ± 8.9), (85.7 ± 5.8), and (94.2 ± 1.9), respectively, indicating that the patients' ability to perform ADL was gradually improving. The ADL in CG were (64.5 ± 9.1), (78.7 ± 6.6), and (89.7 ± 4.6), respectively, indicating the same improvement effect. There were significant differences between the two groups at different time points in AKROM and ADL scores (P < 0.05). The EG had greater flexion angles and ADL scores compared to CG at the same time points (see Table 3).
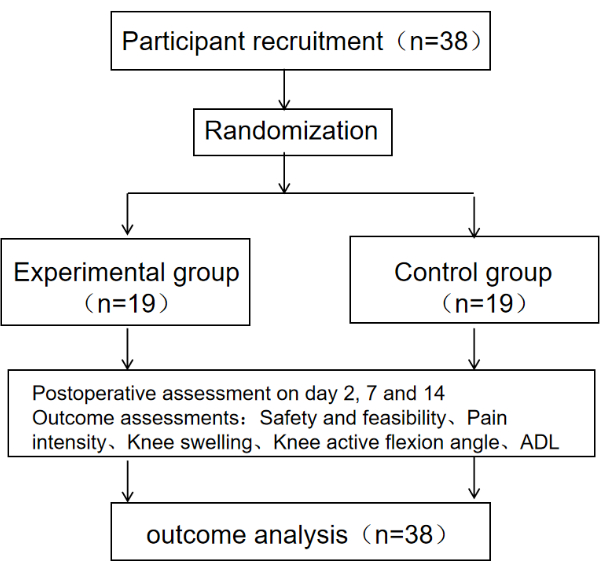
Figure 1: Schematic diagram of the protocol. The schematic diagram of the protocol includes the sample size, grouping, evaluation time, and outcome indicators of the research subjects. Please click here to view a larger version of this figure.

Figure 2: Early weight-bearing standing training. (A–D) The methods and steps of weight-bearing standing. Please click here to view a larger version of this figure.
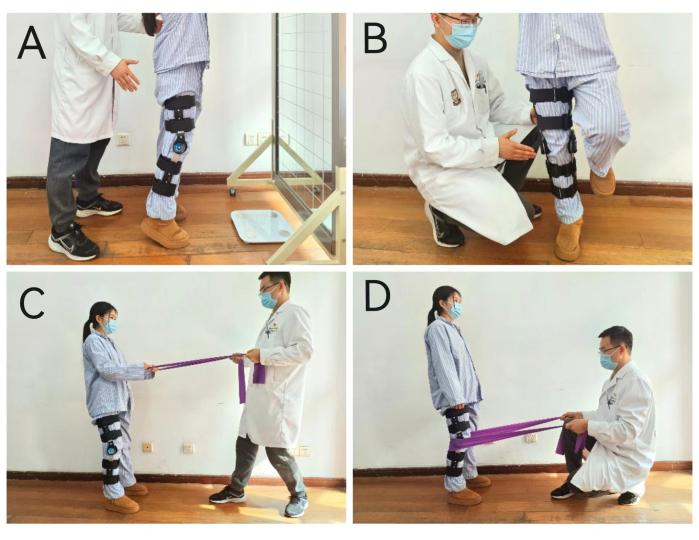
Figure 3: Early weight-bearing balance training. (A–D) Four different methods of balance training. Please click here to view a larger version of this figure.
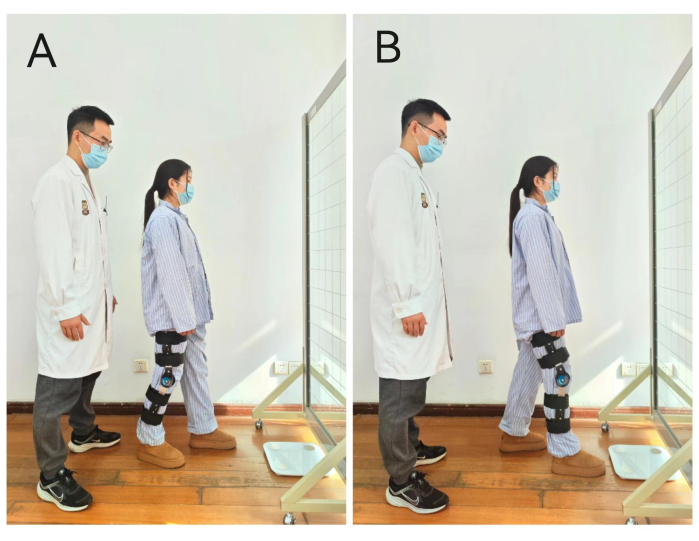
Figure 4: Early weight-bearing gait training. (A,B) Gait training methods with different foot support. Please click here to view a larger version of this figure.
| EG (n=19) | CG (n=19) | P-value | |
| Sex (M/F) | 16/3 | 14/5 | 0.426a |
| Age (years) | 29.8 ± 9.4 | 33.5 ± 7.3 | 0.224b |
| Affected limb (L/R) | 9/10 | 11/8 | 0.516a |
| Graft type (ALL/ARL) | 9/10 | 4/15 | 0.087a |
| Meniscus repair (N/M) | 11/8 | 10/9 | 0.744a |
Table 1: Basic characteristics. This table shows the sample size, gender, age, surgical site, graft type, and meniscus repair degree of the two groups. Data are presented as mean ± SD. Abbreviations: EG = Experimental group; CG = Control group; M = male; F = female; L = left; R = right; ALL =autologous ligament; ARL =artificial ligament; N = no repair; M = mild repair; Superscript a = χ2 test; "b" = t-test.
| G | NRS | DKE | ||||||||||
| Day 2 | Day 7 | Day 14 | Day 2 | Day 7 | Day 14 | |||||||
| Mil | Mod | Sev | Mil | Mod | Sev | Mil | Mod | Sev | ||||
| EG | 2.2±1.3 | 1.1±0.6 | 0.6±0.5 | 4 | 11 | 4 | 9 | 9 | 1 | 12 | 6 | 1 |
| CG | 2.5±1.2 | 1.5±0.8 | 0.8±0.5 | 3 | 10 | 6 | 8 | 10 | 1 | 15 | 3 | 1 |
| P-value | 0.850b | 0.059b | 0.198b | 0.744b | 0.946b | 0.513b | ||||||
Table 2: Pain intensity and degree of knee edema in two groups. This table records the intensity of pain and knee joint edema degree of the two groups at different time points. Data are presented as mean ± SD. Abbreviations: DKE = Degree of knee edema; EG = Experimental group; CG = Control group; Mil = Mild; Mod = Moderate; Sev = Severe; "b" = t-test.
| G | AKROM (degree) | BI | ||||
| Day 2 | Day 7 | Day 14 | Day 2 | Day 7 | Day 14 | |
| EG | 70.5±17.0 | 83.4±13.5 | 98.1±13.0 | 72.8±8.9 | 85.7±5.8 | 94.2±1.9 |
| CG | 56.8±13.1 | 74.7±12.9 | 87.0±10.6 | 64.5±9.1 | 78.7±6.6 | 89.7±4.6 |
| P-value | 0.009b | 0.049b | 0.006b | 0.008b | 0.001b | 0.001b |
Table 3: Active knee flexion range of motion and daily living ability score of two groups after surgery. This table shows the angle of active knee flexion and daily living ability scores of the two groups at different time points. Data are presented as mean ± SD. Abbreviations: AKROM = Active knee flexion range of motion; BI = Barthel index; EG = Experimental group; CG = Control group.
