Material Used in Capnography
One of the obstacles to the utilization of expired CO2 monitoring resides in the disparity of the material used by emergency physicians. To clarify this situation, it is important to distinguish whether the patient is artificially ventilated or breathing spontaneously. As for the rest, the different techniques used for analysis no longer have an implication on clinical results and efficiency.
This statement stands in the case of the traditional distinction between sidestream and mainstream capnography. These two techniques measure CO2 using infrared waves; the sidestream system uses an aspiration pump to transport CO2 from the mouth to the detector situated in the monitor, while the mainstream system measures CO2 directly in a small chamber situated at the mouth of the patient and connected to the monitor by a cable. Traditionally, the sidestream system is used for patients breathing spontaneously as the system is lighter, and the mainstream system, a little bulkier, is connected directly to the endotracheal tube in intubated patients. Technological advances in the last years have fundamentally reduced the differences between mainstream and sidestream systems. New technology is pointing towards the microstream system, which is a sort of ‘enhanced sidestream system’ in which CO2 travels along a thin tube before reaching the chamber where the detector is located, allowing a smaller transition period between the mouth and the detection chamber and thus a capnography curve that is almost synchronized with the passage of air at the mouth. So, let us have a look at what distinguishes the choice of material, as explained in the second half of the video sequence:
- If the physician wishes to monitor a patient in spontaneous ventilation so as to precocely detect apnea (during procedural sedation, or after medical intoxication), then only the form of the curve is essential, the actual value of ETCO2 being of less importance. In this case, he physician can choose between nasal prongs or a capnomask combining oxygen administration and CO2 aspiration, or a thin CO2 aspiration tube that can be placed under a classical mask.
- If the physician wishes to precisely analyse ETCO2 in order to adapt the parameters on a respirator, to verify the correct positioning of an endotracheal tube, or to evaluate the prognosis during cardiac arrest, he must use the material than can be adapted for use with an endotracheal tube (always placed behind the filter so as secretions from the patient do not block the tube).
The Capnography Curve
A typical capnography curve during three expirations is given in Figure 1. The curve regains the x-axis (0 value) at each inspiration, as there is virtually no CO2 in inspired air.
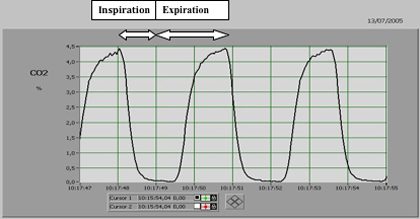
Figure 1: alternance inspiration-expiration
Differences Between PaCO2 and ETCO2
It would be eutopic to believe that non-invasive monitoring of expired CO2 can replace in all circumstances the need for arterial blood gas (ABG) measures, considered to be the gold standard for the measurement of PaCO2. All depends on the indications for the measurement of expired CO2 and the patient’s cardio-respiratory condition. If the indication is the monitoring of respiratory activity to prevent hypoventilation and apnea during sedation, a simple analysis of the curve is sufficient, whatever the value of ETCO2. On the other hand, if the indication is to monitor the adequate ventilation of a head trauma patient with no history of cardio-respiratory disorders, we can expect the ETCO2 value to be close to the PaO2 value, though the necessity of a precise PaCO2 value imposes at least one ABG sample, which also allows us to confirm that indeed ETCO2 is close to PaCO2 in the present case.
Finally, if we are faced with the case of a patient that is intubated and ventilated due to respiratory distress, ETCO2 values will evidently not be a good approximation of PaCO2. The reason is simple; as soon as there is a disturbance in ventilation-perfusion ratios, regardless of what the cardio-pulmonary disorder present is, an obstacle to the correct elimination of CO2 by the lungs is created. As a result, CO2 accumulates in the blood, and naso-buccal elimination is reduced, creating a PaCO2 – ETCO2 gradient. In this circumstance, it is crucial to know the value of PaCO2 before any interpretation of the ETCO2 value.
The first part of the video sequencedescribes the procedure to be followed for interpreting the difference between PaCO2 and ETCO2. We see that the measure of ETCO2 is obtained immediately and in a non-invasive manner, but at this stage cannot allow the adaptation of the respirator’s parameters. This implies having to measure the PaCO2 that can then be compared with the ETCO2. The PaCO2 value remains the referral value for the appreciation of patient ventilation.
- If PaCO2 measured is higher than the desired value, for example 60mmHg instead of 40mmHg, this signifies that the patient is hypoventilated. The respirator’s parameters can then be adapted; either the respiratory rate or the tidal volume can be increased in order to increase the ventilation and thus decrease PaCO2. The objective consists in reducing the ETCO2 by 20mmHg, regardless of the initial ETCO2 value. For example, it can be possible that the ETCO2 value is 50mmHg when the PaCO2 is measured at 60mmHg, due to a PaCO2 -ETCO2 gradient created by the presence of a cardio-respiratory disease. When the adaptation of the respirator’s parameters allows the ETCO2 to drop from 50mmHg to 30mmHg, we can safely suppose that the patient is adequately ventilated with a PaCO2 value having dropped from 60mmHg to 40mmHg.
- Inversely, if the PaCO2 is lower than the target value, the patient is hyperventilated and consequently respiratory rate or tidal volume must be reduced to attain the target value. If PaCO2 is 20 mmHg lower than the targeted value, one has to increase the ETCO2 by 20mmHg through modification of the respirator’s parameters.
Artifacts and Traps in Capnography.
If the technology for CO2 measurement has become reliable in terms of precision, reproducibility, response time and curve quality, it still presents, as for any monitored parameter, certain limits:
- The first limitation is due to lack of correct knowledge concerning the physiopathology of CO2 by the physician, who then is reluctant to use the technique. We hope that this explanation and the video sequences accompanying will help resolve this limitation.
- In the case of the spontaneously breathing patient, the adjunction of oxygenotherapy via the mask will dilute the expired CO2, which will significantly modify the capnogram and the ETCO2 will drop. The video sequence demonstrates this phenomenon.
- If one wishes to monitor for hypoventilation, or an apnea event, during procedural sedation, we expect ETCO2, in correlation to PaCO2, to increase in parallel to hypoventilation of the patient. Paradoxally, a hypoventilation event in a patient breathing spontaneously is translated by a drop in ETCO2, because the patient is then only breathing with a very small tidal volume, which essentially corresponds to the dead volume of the tracheo-bronchal space; and as we know, this space does not participate in gaseous exchange and thus contains very little CO2.
- During mechanical ventilation, the pitfall is that one forgets that ETCO2 does not necessarily reflect PaCO2 (see previous chapter).
