1. Preparation of BCG lux reporter mycobacteria stock
- Grow BCG lux (M. bovis BCG Montreal strain transformed with the shuttle plasmid pSMT1) with shaking at 200rpm to mid-logarithmic phase in Middlebrook 7H9 broth containing 0.2% glycerol, 0.05% tween 80 and 10% ADC enrichment.
- Prepare 1ml of a 1:10 dilution of BCG lux culture in sterile PBS in a luminometer tube (900μl PBS + 100μl BCG lux culture) in duplicate.
- Load tube containing N-decyl aldehyde (luciferase enzyme substrate) onto the back of the machine and ensure the lid is secured and tubes in place.
- Prime luminometer injector with substrate via the prime program, set to inject 100 ucl x 3 into each of 3 empty priming tubes placed in the luminometer.
- Load the 2 tubes into the luminometer and take readings via a program set at injecting 100 ucl of substrate into each tube and read for 20 sec in 1 sec intervals.
- When the stock has reached 1×108 RLU/ml to 2×108 RLU/ml (this takes about 3-4 days of growth), add an equal volume of sterile 30% glycerol to the culture in a 50ml falcon tube and gently mix.
- Aliquot 1.5ml volumes into labeled 2ml screw-cap microtube and store at -80°C.
2. Determining stock RLU/CFU correlation and contents of aliquots
- Add 15ml of Middlebrook 7H9 culture medium with 10% ADC supplement to a 200ml Erlenmeyer flask with a vented cap.
- Add 15μl of hygromycin and 30μl of 20% Tween.
- Remove a vial of BCG lux from the freezer and defrost at room temperature (RT) in the safety cabinet. Add the contents of the vial to the medium and tighten the cap.
- Incubate with shaking at 200rpm at 37°C for 4 days.
- On each day, make up serial 10-fold dilutions (1:10, 1:100, 1:1000, 1:10,000 and 1:100,000) for CFU determination.
- Set up the same dilutions in parallel and duplicate to determine luminescence (see part 1.2-1.6).
- Prepare two 3-compartment plates of Middlebrook 7H11 agar (1 l of liquid medium containing 0.5% glycerol, 10% OADC supplement, 1 ml of 20% Tween and 1 ml of hygromycin).
- Plate out 100μl of each dilution onto a segment of each plate using separate spreaders, distributing the liquid equally across the individual chamber.
- Seal each plate with parafilm, place in a sterile plastic bag, seal with autoclave tape, and incubate at 37°C for 2 weeks with lids facing down.
- Inspect regularly until CFUs appear (2-3 weeks).
- To count colonies, remove the plates from the incubator and place on a colony counter. Calculate the mean for each dilution from the duplicate plates.
- Calculate the RLU/CFU ratio using equivalent RLU and CFU counts for each dilution. The ratio should be between 3 and 5 RLU/CFU.
3. Preparation of BCG lux culture for inoculation into whole blood
- Add 15ml of Middlebrook 7H9 culture medium with 10% ADC supplement to a 200ml Erlenmeyer flask with a vented cap.
- Add 15μl of hygromycin and 30μl of 20% Tween.
- Remove a vial of BCG lux from the freezer and defrost at RT in the safety cabinet. Add the contents of the vial to the medium and tighten the cap.
- Incubate with shaking at 200rpm at 37°C for 2 to 4 days.
- Prepare 1ml of a 1:10 dilution of BCG lux culture in sterile PBS in a luminometer tube (900μl PBS + 100μl BCG lux culture) in duplicate.
- Prime luminometer with substrate (as described above), gently vortex the 2 tubes and load into the luminometer and take readings (as described above).
- Use this reading to dilute down the culture in PBS to give an equivalent of 7×106 RLU (this will give an inoculum of about 2×105 CFU/ml blood and a ratio of BCG to monocytes of about 1:1, assuming a monocyte count of about 2×105 to 4×105 monocytes per ml of blood).
4. Preparation of whole blood
- Take 3 to 5ml of venous blood in a tube containing preservative-free heparin.
- Transfer the blood to a 50ml falcon tube and dilute with an equal volume of RPMI 1640 containing glutamine and 25mM HEPES (no pen/strep).
- Aliquot 900μl of diluted blood in triplicate into sterile bijou tubes for each time point (6 tubes in total: 3 for 0hrs and 3 for 96hrs. Set up additional tubes for additional timepoints, if necessary.
- Aliquot 900μl of Middlebrooks 7H9 culture medium with 10% ADC supplement + 50μg/ml hygromycin (the same medium as used to culture the BCG lux) in duplicate for the growth controls.
- Add 100μl of the diluted BCG lux to each tube of blood, and to the 2 growth control tubes.
- Mix well and place the 3 bijous for the 96hr time-point and the 2 growth controls on their side in the rocking incubator at 37°C, 20 rev/min (CO2 not required).
5. Measuring luminescence (at 0hr and 96hrs)
- Centrifuge the 3 bijous at 2000g for 10 min.
- Carefully remove 300μl of supernatant without disturbing the pellet and place in 2ml screw-cap microtubes to freeze at -80°C for subsequent cytokine analysis.
- Add 300μl of PBS to each bijou to replace the volume of supernatant removed.
- Aspirate the contents of each bijou into the corresponding 50ml falcon tube and add 8ml distilled water to each tube. Begin a timer for 10 min.
Nb: This is a time-sensitive step, and this incubation must not be any longer than 10 min, beginning from when the cells first come into contact with water. - Rinse each bijou with 2ml of distilled water and vortex for 5 seconds before tipping into the corresponding falcon tube.
- At the end of the 10 minute incubation, centrifuge the falcon tubes at 2000g for 10 minutes.
- Decant supernatant into Surfanios disinfectant.
- Add a few glass beads to each pellet and vortex.
- Add 1ml of sterile PBS to each tube and vortex.
- In luminometer tubes, make 1:10 dilutions for each sample in duplicate with PBS (900μl PBS + 100μl sample) and at the 96hr time-point. Make the same dilutions for each of the growth controls.
- Gently vortex the tubes and load into the luminometer and take readings (as described above)
Nb: Readings between triplicates of the same sample should be within 15% of one another.
6. Representative results:
It is important to use bacteria in logarithmic phase of growth for the whole blood lux assays, i.e. grown over 48-72 hours prior to inoculating the samples, as metabolic activity is suboptimal if either straight out of the freezer or in stationary phase. The prior growth should be standardized for a series of experiments to either 48 or 72 hours to avoid variability. Figure 1 shows the growth curve of a representative culture of BCG lux. The doubling time is about 24 hours until stationary phase is reached.
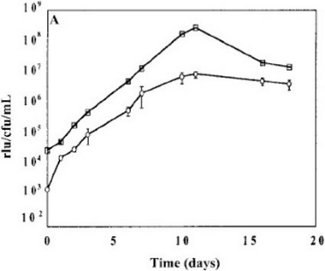
Figure 1. Representative growth curve of BCG lux over 96 hours in 7H9 medium and correlation of RLU and CFU.
Although RLU values always correlate with CFU, the number of RLU corresponding to a single CFU can vary depending on the stock, which is why it is good practice to use the same frozen stock throughout a series of experiments to guarantee a consistent multiplicity of infection (MOI).
Table 1 shows an example of raw date at time of inoculation (T0) and at 96 hours. The growth ratios are calculated using the formula T96/T0, but other time intervals can of course also be measured. It is, however, advisable not to use the cultures beyond 96 hours, as significant cell death occurs.
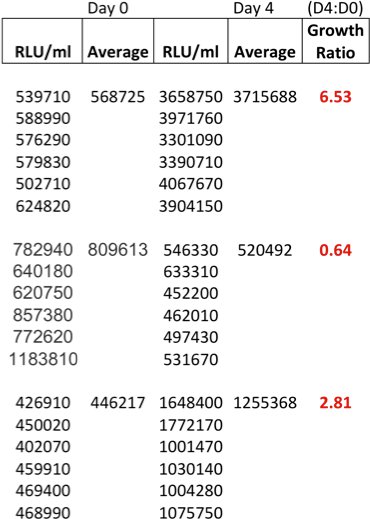
Table 1. Example of raw data at time of inoculation (T0) and at 96 hours (T96) and calculated growth ratios from 3 adult donors.
Depending on the available antigen-specific memory responses and possibly also neutrophil count, growth ratios vary among individuals, as shown here in Figure 2 in the blood of children with and without HIV-infection. On average, young children have higher growth ratios than adults, Tuberculin skin test (TST) +ve individuals have lower growth ratios than TST-ve individuals, and HIV-infected patients have high growth ratios due to the deficiency of CD4 T cell population, one of the key mediators of cellular immune responses to mycobacteria.
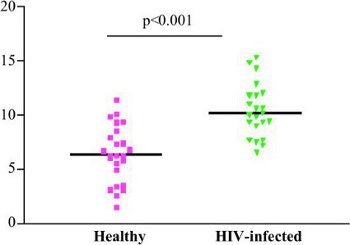
Figure 2. Inter-donor variability: Growth ratios of T0 versus 96 hours for a set of patients, depending on underlying HIV status.
Reproducibility of growth ratios over a period of time is shown in Figure 3, which summarises results from 64 donors bled twice over a period of 12 months and from a single donor bled repeatedly for control experiments. Potential causes of variability could be changes in mycobacterial sensitization or variability within levels of host cytokines, as observed in many bioassays.
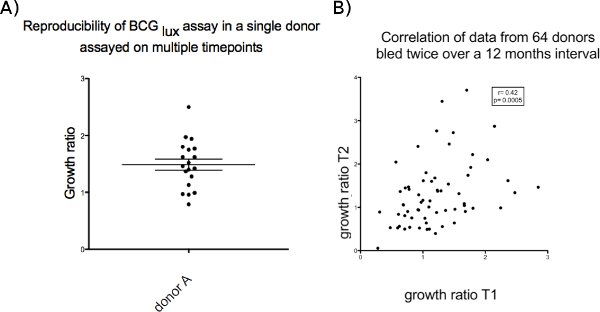
Figure 3. (a) Single donor on 12 occasions over 12 months. (b) multiple (64) donors on 2 occasions over 12 months.
