Determination of the Transport Rate of Xenobiotics and Nanomaterials Across the Placenta using the ex vivo Human Placental Perfusion Model
Summary
The ex vivo dual recirculating human placental perfusion model can be used to investigate the transfer of xenobiotics and nanoparticles across the human placenta. In this video protocol we describe the equipment and techniques required for a successful execution of a placenta perfusion.
Abstract
Decades ago the human placenta was thought to be an impenetrable barrier between mother and unborn child. However, the discovery of thalidomide-induced birth defects and many later studies afterwards proved the opposite. Today several harmful xenobiotics like nicotine, heroin, methadone or drugs as well as environmental pollutants were described to overcome this barrier. With the growing use of nanotechnology, the placenta is likely to come into contact with novel nanoparticles either accidentally through exposure or intentionally in the case of potential nanomedical applications. Data from animal experiments cannot be extrapolated to humans because the placenta is the most species-specific mammalian organ 1. Therefore, the ex vivo dual recirculating human placental perfusion, developed by Panigel et al. in 1967 2 and continuously modified by Schneider et al. in 1972 3, can serve as an excellent model to study the transfer of xenobiotics or particles.
Here, we focus on the ex vivo dual recirculating human placental perfusion protocol and its further development to acquire reproducible results.
The placentae were obtained after informed consent of the mothers from uncomplicated term pregnancies undergoing caesarean delivery. The fetal and maternal vessels of an intact cotyledon were cannulated and perfused at least for five hours. As a model particle fluorescently labelled polystyrene particles with sizes of 80 and 500 nm in diameter were added to the maternal circuit. The 80 nm particles were able to cross the placental barrier and provide a perfect example for a substance which is transferred across the placenta to the fetus while the 500 nm particles were retained in the placental tissue or maternal circuit. The ex vivo human placental perfusion model is one of few models providing reliable information about the transport behavior of xenobiotics at an important tissue barrier which delivers predictive and clinical relevant data.
Introduction
The placenta is a complex organ which is responsible for the exchange of oxygen, carbon dioxide, nutrients and waste products and at the same time able to keep the two blood circuits of the mother and the growing fetus separated from each other. Additionally, it prevents rejection of the child by the maternal immune system and secretes hormones to maintain pregnancy. The cellular barrier is formed by the cytotrophoblast cells which fuse and form a true syncytium without lateral cell membranes 4,5. The whole placenta is organized in several cotyledons, which contain one fetal villous tree and represent one functional unit of the placenta.
The study of the placental barrier function was intensified with the discovery of the thalidomide induced malformations in the 1960’s. For obvious reasons translocation studies with pregnant women cannot be performed. Consequently, various alternative models have been developed 6,7. The most promising and probably most clinical relevant model is the ex vivo human placental perfusion model developed by Panigel and co-workers 2,3.
Many women are exposed to different xenobiotics such as drugs or environmental pollutants during their pregnancy 8. For some drugs which were already administered regularly during pregnancy, in vivo studies can be performed by comparison of the maternal blood concentration with that in umbilical cord blood. However, generally there is only limited information about the pharmacokinetics and -dynamics in the fetus and the teratogenicity of these substances.
For example opiates like heroin easily cross the placental barrier and can lead to intrauterine growth restriction, preterm delivery or spontaneous abortion 9,10. So, in case of missing abstinence during pregnancy a replacement therapy with methadone is recommended. The ex vivo human placental perfusion model revealed that the transfer of methadone into the fetal circulation is negligible 11, which correlates well with the calculated cord blood-to-maternal blood concentration ratio after delivery 12.
Nanotechnology is a growing field especially in medicine. So, beneath the naturally occurring fine (< 2.5 μm in diameter) and ultrafine particles (< 0.1 μm in diameter) in fumes of forest fires, volcano eruptions and in desert dust, exposure to engineered nanomaterials (at least one dimension < 0.1 μm 13) is increasing. This raised questions about the toxicological potential of engineered nanomaterials. Although no human hazard could be proved yet, there are principal experimental studies indicating that engineered nanoparticles can cause adverse biological responses leading to toxicological outcomes 14. Recently, some studies indicated that prenatal exposure to air pollution is linked to a higher respiratory need and airway inflammation in newborns and children 15,16. In addition, small nanoparticles might be used as drug carriers to specifically treat either the fetus or the mother. Therefore, it becomes evident that extensive studies of distinct xenobiotics or nanomaterials and their ability to cross the placental barrier are required. An actual overview on the current studies on placental permeability to engineered nanomaterials is summarized in Menezes et al. 2011 17 and Buerki-Thurnherr et al. 2012 7.
The ex vivo dual recirculating human placental perfusion model provides a controlled and reliable system for studying the placental transport of various endogenous and exogenous compounds 3,11,12,18,19 and a wide range of other functions of the placenta like mechanisms responsible for the development of pathological states like preeclampsia 20-22. In this protocol we focus mainly on the set up, handling and method that allow the study of accumulation, effects and translocation rates of a broad set of xenobiotics or nanoparticles.
Protocol
1. Preparing the Perfusion System
- Set up the perfusion system consisting of a water bath, a perfusion chamber, two columns for oxygenation, two peristaltic pumps, two bubble traps, two flow heaters and one pressure sensor (Figure 1). Connect these components with tubing sections composed of silicone and polyvinyl chloride materials according to the scheme in Figure 2. Finally there are two circuits representing the fetal and maternal circuit, respectively.
- Turn on the water bath, the flow heaters and the heating for the perfusion chamber. The temperature should be 37 °C.
- Warm up the perfusion medium (NCTC-135 tissue culture medium diluted 1:2 with Earle’s buffer (6.8 g/L sodium chloride, 0.4 g/L potassium chloride, 0.14 g/L monosodium phosphate, 0.2 g/L magnesium sulfate, 0.2 g/L calcium chloride, 2 g/L glucose) supplemented with glucose (1 g/L), dextran 40 (10 g/L), bovine serum albumin (10 g/L), sodium heparin (2,500 IU/L), amoxicilline (250 mg/L) and sodium bicarbonate (2.2 g/L); pH 7.4) in the water bath.
- Consecutively rinse the arterial systems of the fetal and maternal circuit with a) 200 ml distilled water, b) 50 ml 1% sodium hydroxide, c) 1% phosphoric acid and d) again 200 ml distilled water (flow rate: 15 – 20 ml/min).
- Connect the fetal cannula (Ø 1.2 mm; blunt needle should be attached to a modified winged needle infusion set) to the fetal arterial tubing.
- Rinse the arterial systems of the fetal and maternal circuit with perfusion medium until all tubes contain medium (flow rate: 15-20 ml/min). During this step fill up the bubble traps and remove all bubbles downstream of the trap. Then stop the pumps. It is really important that the afferent arterial tubes are always free of bubbles; otherwise after cannulation especially the fine fetal vessels can rupture.
- Turn on the gas flow. The maternal circuit is oxygenated with 5% carbon dioxide and 95% synthetic air and the fetal circuit with 5% carbon dioxide and 95% nitrogen.
- Start the recording of the pressure sensor.
2. Cannulating the Placenta
- Obtain intact placentae from uncomplicated term pregnancies after primary cesarean section. Written consent has to be given (was obtained in the case of our studies) by the mothers before delivery and the study has to be approved by the local ethics committee (was the case in our studies). First visual control should be done by midwives to assure a healthy and intact placenta.
- Cannulation of the placenta is a critical step! During perfusion every small disruption in the tissue can lead to a leak between the maternal and fetal circulation. The placenta has to be obtained within 30 min after delivery.
- Select an intact cotyledon at the marginal zone of the placenta without visible disruptions on the maternal side. At the chorionic plate, tie up both associated branches of the umbilical artery and vein upstream to the later cannulation side (towards the umbilical cord) by using surgical suture material. Make always two knots.
- Cannulate the fetal artery first. The fetal placental arteries are always smaller and thinner than the veins.
- Make a suture around the fetal artery, but do not tie it up immediately. Hold the vessel with a forceps, cut the vessel carefully and put the small cannula (Ø 1.2 mm) in the artery. Then tie up the suture (two knots).
- Proceed with the fetal vein in the same manner but use a bigger cannula (Ø 1.5-1.8 mm; blunt needle should be attached to a modified winged needle infusion set).
- Turn on the fetal pump (2 ml/min). If there is no visible leak and blood emanates out of the fetal vein cannula, slowly increase the flow up to 4 ml/min. Observe the pressure in the fetal artery, it should not exceed 70 mmHg. If fluid leaks out at the fetal or maternal cannula fix them with another suture.
- Place the placenta on the tissue holder with the fetal side up and pull the placental membrane and tissue over the spikes. In the end the perfused cotyledon should be in the middle of the hole in the tissue holder.
- Stabilize the part where only the membrane holds the placenta with a silicone membrane (Ø 1 mm) or alternatively two parafilm pieces.
- Assemble the complete tissue holder, tighten the screws and cut the overhanging tissue. Please note that the venous and arterial cannulae are not pinched but instead lay in the small channels of the tissue holder.
- Turn the tissue holder upside down, put it into the perfusion chamber and add the cover. Now, the maternal side should be at the top. Check always if the fetal circuit is still intact and the medium is flowing out of the fetal vein tubing.
- Turn on the maternal pump (12 ml/min). Introduce the three blunt cannulae (Ø 0.8 mm) at the end of the maternal artery tube into the intervillous space by penetrating the decidual plate. To return the perfusate to the maternal circuit put one tube as venous drain which is also connected with the maternal pump to the lowest position in the upper part of the perfusion chamber.
- Connect the fetal vein cannula to the fetal vein tube.
3. Executing the Pre- and Experimental Phase of Perfusion
- To allow the tissue to recover from the ischemic period after delivery and to flush out the blood in the intervillous space, an open pre-phase of 20 min is necessary. That means the maternal and fetal vein are not leading back to the arterial reservoir containing the perfusion medium. Collect the fetal and maternal venous outflow in a bottle and discard it after the pre-phase.
- To assess the integrity of the perfusion perform another pre-phase of 20 min but in a closed circuit. Use two separate reservoirs with perfusion medium for the fetal and maternal circuit and close the circuits by leading the fetal venous outflow back in the fetal reservoir and the maternal venous outflow back in the maternal reservoir.
- For the main perfusion experiment prepare two flasks with 120 ml perfusion medium (one for the maternal and one for the fetal reservoir). Add the radiolabeled 14C-antipyrine (4 nCi/ml; serves as positive control; CAUTION: radioactive substance) and the fluorescently labeled xenobiotic or nanoparticles which one wants to analyze to the maternal reservoir. Mix the maternal perfusate well.
- Start the experiment by exchanging the pure perfusion medium with the two prepared flasks (fetal and maternal reservoirs). Close the circuits by leading the fetal venous outflow back in the fetal reservoir and the maternal venous outflow back in the maternal reservoir.
- Continue the perfusion for 6 hr and take samples regularly. Always resuspend the medium in the fetal and maternal reservoir before withdrawal.
- Control the pressure in the fetal artery (should not exceed 70 mmHg), pH in both circuits (should be in a physiological range 7.2-7.4) and the volume of both reservoirs (fetal volume loss should not exceed 4 ml/hr) during perfusion. If necessary adjust the pH values using either hydrochloric acid or sodium hydroxide.
- If the volume loss in the fetal reservoir exceeds 4 ml/hr there is a leak in the tissue and one has to stop the perfusion. The success rate of a perfusion for 6 hr without leak is about 15-20%.
- Stop the perfusion after 6 hr. Turn out the pumps, water bath, flow heaters and gas flow.
- Remove the placenta from the tissue holder, cut the perfused cotyledon (brighter than the unperfused tissue) and weigh it.
- Take samples from unperfused (part of the placenta which was cut in the beginning; could be already taken during the pre-phase) and perfused tissue (each about 1 g) and store them at -20 °C until homogenization or in liquid nitrogen for later analysis. Fix another tissue sample in 4% formalin for histopathological evaluation. The samples should include all layers of the placenta.
- Clean the tubes after perfusion by successively rinsing the arterial systems of the fetal and maternal circuit with a) 200 ml distilled water, b) 50 ml 1% sodium hydroxide, c) 50 ml 1% phosphoric acid and d) again 200 ml distilled water (flow: 15-20 ml/min).
The entire working procedure of the placenta perfusion experiment is depicted in Figure 3.
4. Analyzing the Samples
- Centrifuge the perfusate samples for 10 min at 800 x g before analysis to remove residual erythrocytes. Take the supernatant for the further analysis. The samples can be left overnight at 4 °C. For the analysis of leptin and hCG production the samples can be stored at -20 °C.
- To evaluate the permeability of the placenta analyze the 14C-antipyrine by liquid scintillation. Mix 300 μl of the fetal and maternal samples with 3 ml scintillation cocktail and measure for 5 min in a beta counter.
- To assess the transfer of the fluorescent nanoparticles or the xenobiotic of interest read the fluorescence at 485 nm excitation and 528 nm emission in a microplate reader (indicated wavelengths are for analysis of the yellow green label which we used for the nanoparticles).
- To determine the viability of the placental tissue during perfusion measure the glucose consumption and lactate production in the fetal and maternal circuit with an automated blood gas system. Additionally, evaluate the production of the placental hormones human choriongonadotropin (hCG) and leptin in the homogenized tissue samples and the perfusates by enzyme-linked immunosorbent assay (ELISA).
Representative Results
Figure 4A shows the perfusion profiles of small polystyrene particles (80 nm) which were transported across the placenta compared to bigger polystyrene particles (500 nm) which were not transferred to the fetal compartment. Each data point represents the mean particle concentration to the given time point of at least 3 independent experiments. For polystyrene nanoparticles the placental transfer is size-dependent 19. After 3 hr of placenta perfusion already 20-30% of the initially added 80 nm polystyrene particles were transferred from the maternal to the fetal circuit, while the 500 nm polystyrene particles were not appearing in the fetal circuit even after 6 hr of perfusion. Nevertheless, the maternal concentration of the 500 nm particles is decreasing. Fluorescence images on histological section of the tissue after perfusion showed that these particles accumulate in the villi of the placenta (data not shown). Figure 4B depicts a characteristic perfusion profile of the radiolabeled 14C-antipyrine. Antipyrine as a small lipophilic molecule is distributed over the placental barrier via passive diffusion and serves as control for the integrity of the circuits. After 4-6 hr of perfusion an equilibrium between the fetal and maternal antipyrine concentration should be built 23. To assess and compare the placental transport rate of xenobiotics the fetal-to-maternal drug concentration (F/M) ratio is usually displayed (Figure 5).
Through the analysis of lactate and placental hormone (human choriongonadotropin and leptin) production as well as glucose consumption the viability and functionality of the placental tissue during the perfusion could be monitored (Figure 6). The values for the perfusions with xenobiotic should always be in the same range as the values from control perfusion without xenobiotic. In addition, histopathological evaluation of the perfused placental tissue could be performed. A comparison with non-perfused placental tissue could then reveal pathological changes due to perfusion (e.g. bacterial contamination) and therefore could serve as another quality control parameter.
Further representative results obtained with the ex vivo dual recirculating human placental perfusion model were published recently 11,19.
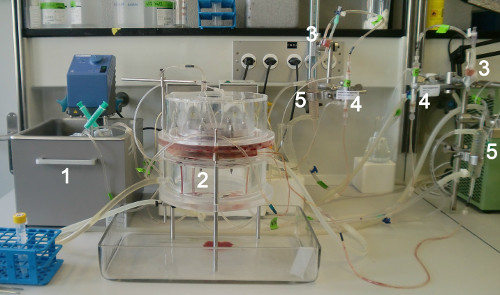
Figure 1. Ex vivo human placental perfusion set-up. 1) Water bath with maternal and fetal reservoirs, 2) perfusion chamber, 3) bubble trap, 4) oxygenator columns, and 5) flow heater.
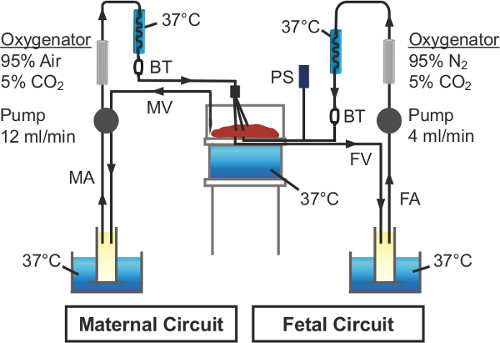
Figure 2. Schematic illustration of the ex vivo human placental perfusion model. FA: fetal artery; FV: fetal vein; MA: maternal artery; MV: maternal vein; BT: bubble trap; PS: pressure sensor
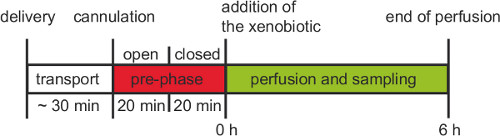
Figure 3. Working procedure of an ex vivo human placental perfusion experiment. After delivery the placenta has to be cannulated within 30 min. Before the 6 hr experimental phase with recirculation an open pre-phase and closed pre-phase should be performed for at least 20 min each.
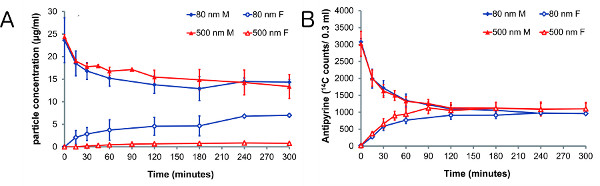
Figure 4. Perfusion profiles of polystyrene particles and 14C-antipyrine 19. Perfusion profile of polystyrene particles in the sizes 80 nm (n=4) and 500 nm (n=3). Initially 25 μg/ml particles and 4.2 nCi/ml 14C-antipyrine were added to the maternal circuit. The amount of particles (A) and 14C-antipyrine (B) were measured in the maternal (M, solid symbols) and fetal (F, open symbols) circuits after the indicated time points. Displayed is the mean concentration ± SE. Click here to view larger figure.
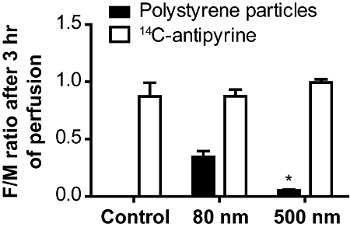
Figure 5. Size-dependent transfer of polystyrene particles across the human placenta 19. The ratios between fetal and maternal concentrations of 14C-antipyrine and polystyrene particles were calculated after 180 min of placenta perfusion. Data represent the mean ± SE of at least 3 independent experiments. The control column depicts perfusions without particles but with 14C-antipyrine. (* p < 0.05 compared with 80 nm ratio value).
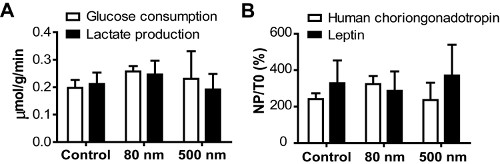
Figure 6. Viability of the placental tissue during perfusion 19. (A) Glucose consumption and lactate production in the perfused placenta. Displayed is the sum of changes in total content in the circuits (fetal and maternal) over time divided by the weight of the perfused cotyledon. (B) Normalized net production (NP divided by initial tissue content T0) of the placental hormones human choriongonadotropin and leptin. Data represent the mean ± SE of at least 3 independent experiments.
Discussion
Beneath the dual recirculating perfusion showed here, there are several other experimental configurations possible depending on the question which has to be answered. Particularly open placental perfusions are commonly used to assess the drug clearance at steady-state concentration 3. The recirculating perfusion set-up can be also applied to confirm active transport of endogenous or exogenous substances. For this approach the same concentration of the xenobiotic has to be added to the maternal and the fetal circulation. Assumed that there is active transport against the concentration gradient, accumulation of the test substance in either one of the both circuits may be observed 24. Of note, the addition of the test substance only to the fetal circuit is also feasible and can reveal the mechanism of transport across the placental barrier of this particular substance 25.
The protocol has evolved over time and can vary between different research groups especially concerning the flow rate, composition of perfusion medium, form of oxygenation and heating 26,27. Especially the flow rate can influence the time at which transplacental transfer occurs. To control this, the addition of a passively transported reference compound like antipyrine is important. The transfer rate of the xenobiotic can be always compared to the transfer rate of antipyrine (F/M ratio should be above 0.75) 26. Since the antipyrine transfer is mainly limited by the flow and exchange surface, this comparison takes differences in the flow and the size of the perfused cotyledon into account which could vary between the experiments. In addition, FITC-dextran could be added to the fetal circuit to serve as control for the integrity of the barrier 26. Fetal volume loss is also used as marker for the barrier integrity. Usually a fetal fluid loss up to 4 ml/hr is allowed 28, but there is no generally accepted limit.
Obviously, there are some disadvantages of the ex vivo human placental perfusion method like inter-individual variations and a low success rate (15-20%). Moreover, a perfusion period of 6 hr cannot simulate a chronic drug treatment and therefore can’t completely exclude the transfer of a xenobiotic after long-term exposure. Another limitation of the model is that mainly the transplacental transfer at term is assessed while the transport rate at early gestational ages when the barrier is thicker remains still unknown. Indeed, perfusion of first trimester placentae is possible but the availability of these placentae is rather limited. Nevertheless, up to now the ex vivo placental perfusion method is the only model to study the transport of various xenobiotics or nanoparticles in organized human placental tissue. While toxicodynamics in the ex vivo human perfusion model can be analyzed only in the placental tissue, animal experiments can indeed provide also information about the embryotoxicity. Though, because of the anatomic differences of the placental barrier between humans and rodents these results cannot be extrapolated to humans 4,5. Another possibility to investigate transplacental transfer may be cell culture models like primary cytotrophoblasts, choriocarcinoma cell lines, isolated plasma membrane vesicles or placental tissue explants 29. The most used model is the BeWo cell line; these cells are derived from a malignant gestational choriocarcinoma and can form a confluent monolayer on a permeable membrane, so transport studies can be performed. Results of transport studies using the BeWo cell model correlate well with results obtained in the ex vivo human placental perfusion 30. However, to study the details of drug transport (e.g. contribution of a specific transport protein) and metabolism, the BeWo cell model may be more feasible primarily because it is easier to handle and susceptible to manipulation like expression of genetically altered transporters or enzymes, but regarding general drug transfer studies the reliability of this model is limited. It lacks blood flow and the integrity of the monolayer has to be evaluated carefully since it depends on several factors like cell culture conditions, seeding density, exposure duration and the membrane insert 6,29.
Different xenobiotics and also nanoparticles bind to various plasma proteins which can significantly influence the transplacental transfer 31; considering the binding to plasma proteins is therefore important. The perfusion medium contains bovine serum albumin, the most frequent plasma protein. Recently, a study showed that the transfer ratios of various substances obtained with the ex vivo human placental perfusion model correlate well with the in vivo cord blood to maternal blood concentration ratios when the transfer ratios were adjusted according to the extent of plasma protein binding 12.
Overall, the ex vivo placental perfusion model is a valid and reliable method to study the transport across the human placenta and to predict the in vivo transplacental passage of xenobiotics and nanoparticles.
Declarações
The authors have nothing to disclose.
Acknowledgements
This work is financially supported by the Swiss National Foundation, (NRP 64 program, grant no 4064-131232).
Materials
| Name of the Reagent | Company | Catalogue Number | Comments (optional) |
| NCTC-135 medium | ICN Biomedicals, Inc. | 10-911-22C | could be replaced by Medium 199 from Sigma (M3769) |
| Sodium chloride (NaCl) | Sigma-Aldrich, Fluka | 71381 | |
| Potassium chloride (KCl) | Hospital pharmacy | also possible: Sigma (P9541) | |
| Monosodium phosphate (NaH2PO4 · H2O) | Merck | 106346 | |
| Magnesium sulfate (MgSO4 · H2O) | Sigma-Aldrich, Fluka | 63139 | |
| Calcium chloride (CaCl, anhydrous) | Merck | 102388 | |
| D(+) Glucose (anhydrous) | Sigma-Aldrich, Fluka | 49138 | |
| Sodium bicarbonate (NaHCO3) | Merck | 106329 | |
| Dextran from Leuconostoc spp. | Sigma-Aldrich | 31389 | |
| Bovine serum albumin (BSA) | Applichem | A1391 | |
| Amoxicilline (Clamoxyl) | GlaxoSmithKline AG | 2021101A | |
| Sodium heparin | B. Braun Medical AG | 3511014 | |
| Sodium hydoxide (NaOH) pellets | Merck | 106498 | CAUTION: corrosive |
| Ortho-phosphoric acid 85% (H3PO4) | Merck | 100573 | CAUTION: corrosive |
| Maternal gas mixture: 95% synthetic air, 5% CO2 | PanGas AG | ||
| Fetal gas mixture: 95% N2, 5% CO2 | PanGas AG | ||
| Antipyrine (N-methyl-14C) | American Radiolabeled Chemicals, Inc. | ARC 0108-50 μCi | CAUTION: radioactive material (specific activity: 55mCi/mmol) |
| Scintillation cocktail (IrgaSafe Plus) | Zinsser Analytic GmbH | 1003100 | |
| Polystyrene particles 80 nm | Polyscience, Inc. | 17150 | |
| Polystyrene particles 500 nm | Polyscience, Inc. | 17152 | |
| EQUIPMENT | |||
| Water bath | VWR | 462-7001 | |
| Thermostat | IKA-Werke GmbH & Co. KG | 3164000 | |
| Peristaltic pumps | Ismatec | ISM 833 | |
| Bubble traps (glass) | UNI-GLAS Laborbedarf | ||
| Flow heater | UNI-GLAS Laborbedarf | ||
| Pressure sensor + Software for analyses | MSR Electronics GmbH | 145B5 | |
| Notebook | Hewlett Packard | ||
| Miniature gas exchange oxygenator | Living Systems Instrumentation | LSI-OXR | |
| Tygon Tube (ID: 1.6 mm; OD: 4.8 mm) | Ismatec | MF0028 | |
| Tubes for pumps (PharMed BPT; ID: 1.52 mm) | Ismatec | SC0744 | |
| Blunt cannulae (Ø 0.8 mm) | Polymed Medical Center | 03.592.81 | |
| Blunt cannulae (Ø 1.2 mm) | Polymed Medical Center | 03.592.90 | |
| Blunt cannulae (Ø 1.5 mm) | Polymed Medical Center | 03.592.94 | |
| Blunt cannulae (Ø 1.8 mm) | Polymed Medical Center | 03.952.82 | |
| Parafilm | VWR | 291-1212 | |
| Perfusion chamber with tissue holder (plexiglass) | Internal technical department | Similar equipment is available from Hemotek Limited, UK | |
| Surgical suture material (PremiCron) | B. Braun Medical AG | C0026005 | |
| Winged Needle Infusion Set (21G Butterfly) | Hospira, Inc. | ASN 2102 | |
| Multidirectional stopcock (Discofix C-3) | B. Braun Medical AG | 16494C | |
| Surgical scissors | B. Braun Medical AG | BC304R | |
| Dissecting scissors | B. Braun Medical AG | BC162R | |
| Needle holder | B. Braun Medical AG | BM200R | |
| Dissecting forceps | B. Braun Medical AG | BD215R | |
| Automated blood gas system | Radiometer Medical ApS | ABL800 FLEX | |
| Multi-mode microplate reader | BioTek | Synergy HT | |
| Liquid scintillation analyzer | GMI, Inc. | Packard Tri-Carb 2200 | |
| Scintillation tubes 5.5 ml | Zinsser Analytic GmbH | 3020001 | |
| Tissue Homogenizer | OMNI, Inc. | TH-220 | |
| pH meter + electrode | VWR | 662-2779 |
Referências
- Ala-Kokko, T. I., Myllynen, P., Vahakangas, K. Ex vivo perfusion of the human placental cotyledon: implications for anesthetic pharmacology. Int. J. Obstet. Anesth. 9, 26-38 (2000).
- Panigel, M., Pascaud, M., Brun, J. L. Radioangiographic study of circulation in the villi and intervillous space of isolated human placental cotyledon kept viable by perfusion. J. Physiol. (Paris). 59, 277 (1967).
- Schneider, H., Panigel, M., Dancis, J. Transfer across the perfused human placenta of antipyrine, sodium and leucine. Am. J. Obstet. Gynecol. 114, 822-828 (1972).
- Enders, A. C., Blankenship, T. N. Comparative placental structure. Adv. Drug Deliv. Rev. 38, 3-15 (1999).
- Takata, K., Hirano, H. Mechanism of glucose transport across the human and rat placental barrier: a review. Microsc. Res. Tech. 38, 145-152 (1997).
- Saunders, M. Transplacental transport of nanomaterials. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 1, 671-684 (2009).
- Buerki-Thurnherr, T., von Mandach, U., Wick, P. Knocking at the door of the unborn child: engineered nanoparticles at the human placental barrier. Swiss Med. Wkly. 142, w13559 (2012).
- Gendron, M. P., Martin, B., Oraichi, D., Berard, A. Health care providers’ requests to Teratogen Information Services on medication use during pregnancy and lactation. Eur. J. Clin. Pharmacol. 65, 523-531 (2009).
- Burns, L., Mattick, R. P., Lim, K., Wallace, C. Methadone in pregnancy: treatment retention and neonatal outcomes. Addiction. 102, 264-270 (2007).
- von Mandach, U. Drug use in pregnancy. Ther. Umsch. 62, 29-35 (2005).
- Malek, A., Obrist, C., Wenzinger, S., von Mandach, U. The impact of cocaine and heroin on the placental transfer of methadone. Reprod. Biol. Endocrinol. 7, 61 (2009).
- Hutson, J. R., Garcia-Bournissen, F., Davis, A., Koren, G. The human placental perfusion model: a systematic review and development of a model to predict in vivo transfer of therapeutic drugs. Clin. Pharmacol. Ther. 90, 67-76 (2011).
- International Organization for Standardization (ISO). Technical Specification (ISO/TS) 27687. Nanotechnologies – Terminology and definitions for nano-objects – Nanoparticles, nanofibre and nanoplate. , (2008).
- Pietroiusti, A. Health implications of engineered nanomaterials. Nanoscale. 4, 1231-1247 (2012).
- Latzin, P., Roosli, M., Huss, A., Kuehni, C. E., Frey, U. Air pollution during pregnancy and lung function in newborns: a birth cohort study. Eur. Respir. J. 33, 594-603 (2009).
- Lacasana, M., Esplugues, A., Ballester, F. Exposure to ambient air pollution and prenatal and early childhood health effects. Eur. J. Epidemiol. 20, 183-199 (2005).
- Menezes, V., Malek, A., Keelan, J. A. Nanoparticulate drug delivery in pregnancy: placental passage and fetal exposure. Curr. Pharm. Biotechnol. 12, 731-742 (2011).
- Muhlemann, K., Menegus, M. A., Miller, R. K. Cytomegalovirus in the perfused human term placenta in vitro. Placenta. 16, 367-373 (1995).
- Wick, P., et al. Barrier capacity of human placenta for nanosized materials. Environ. Health Perspect. 118, 432-436 (2010).
- Dancis, J. Why perfuse the human placenta. Contrib Gynecol. Obstet. 13, 1-4 (1985).
- May, K., et al. Perfusion of human placenta with hemoglobin introduces preeclampsia-like injuries that are prevented by alpha1-microglobulin. Placenta. 32, 323-332 (2011).
- Guller, S., et al. Protein composition of microparticles shed from human placenta during placental perfusion: Potential role in angiogenesis and fibrinolysis in preeclampsia. Placenta. 32, 63-69 (2011).
- Challier, J. C. Criteria for evaluating perfusion experiments and presentation of results. Contrib. Gynecol. Obstet. 13, 32-39 (1985).
- Kraemer, J., Klein, J., Lubetsky, A., Koren, G. Perfusion studies of glyburide transfer across the human placenta: implications for fetal safety. Am. J. Obstet. Gynecol. 195, 270-274 (2006).
- leal, J. K., et al. Modification of fetal plasma amino acid composition by placental amino acid exchangers in vitro. J. Physiol. 582, 871-882 (2007).
- athiesen, L., et al. Quality assessment of a placental perfusion protocol. Reprod. Toxicol. 30, 138-146 (2010).
- Myllynen, P., et al. Preliminary interlaboratory comparison of the ex vivo dual human placental perfusion system. Reprod Toxicol. 30, 94-102 (2010).
- Malek, A., Sager, R., Schneider, H. Maternal-fetal transport of immunoglobulin G and its subclasses during the third trimester of human pregnancy. Am. J. Reprod. Immunol. 32, 8-14 (1994).
- Prouillac, C., Lecoeur, S. The role of the placenta in fetal exposure to xenobiotics: importance of membrane transporters and human models for transfer studies. Drug Metab. Dispos. 38, 1623-1635 (2010).
- Poulsen, M. S., Rytting, E., Mose, T., Knudsen, L. E. Modeling placental transport: correlation of in vitro BeWo cell permeability and ex vivo human placental perfusion. Toxicol. In Vitro. 23, 1380-1386 (2009).
- Mathiesen, L., Rytting, E., Mose, T., Knudsen, L. E. Transport of benzo[alpha]pyrene in the dually perfused human placenta perfusion model: effect of albumin in the perfusion medium. Basic Clin. Pharmacol. Toxicol. 105, 181-187 (2009).
