The skeletal muscle procedure as described follows the guidelines of the Appalachian State University Institutional Review Board.
NOTE: The team consists of an operator (Ph.D. or M.D. trained in the biopsy technique), and at least one, but ideally, three or more technicians. The operator is responsible for conducting and overseeing all aspects of the skeletal muscle biopsy procedure. One technician (technician #1) is immediately responsible for assisting the operator with all aspects of muscle extraction. This includes being the “non-sterile hands” and applying suction with a sterile syringe. A second technician (technician #2) engages in conversation with subject and massages the subject’s opposite leg during procedure to minimize the subject's anxiety. The third technician (technician #3) is responsible for handling and processing the skeletal muscle sample. Downstream analytical measures dictate how many additional technicians are required for processing/preparing the skeletal muscle sample.
1. Subject Preparation
- Gather, prepare, and organize the materials specified for the muscle biopsy procedure (Table 1). Decontaminate and sterilize the Bergström needle (outer cannula and inner trocar) and the plunger according to standard practice16.
- Review the consent form with the subject. The skeletal muscle biopsy portion of the Consent to Participate form used at Appalachian State University is provided in online supplement 1.
- Talk to the subject about the general aspects of the muscle biopsy procedure with a focus on possible risks of the procedure, skin preparation, application of the anesthetic, typical sensations. Instruct the subject to carefully read the Consent to Participate form and sign it to confirm that the study design and procedures are understood.
- Confirm that the subject is not allergic to “___caine”-type medications (e.g., lidocaine).
- Instruct the subject to lie supine on a padded table with the thigh exposed. Place two disposable absorbent underpads with plastic backing under the subject’s leg. Position the leg in a relaxed manner with a small towel roll under the heel, such that the knee is fully extended (elevated ~1 cm), thus placing the vastus lateralis in a shortened position.
- Have the operator instruct the subject to momentarily contract the exposed thigh muscle so that the biopsy site can be visualized. Note: The vastus lateralis biopsy site is just anterior to the fascia lata (illiotibial band), approximately one-third of the distance between the top of the patella and the greater trochanter7.
- Have the operator mark just below (~0.5 cm) the incision site with a fine point permanent marker.
- Have the operator determine the approximate skinfold thickness by pinching the skinfold.
- Have the operator and technicians wash their hands with soap and warm water and don disposable gloves.
- Have the operator remove the hair from a region ~15 cm x 15 cm around the biopsy site (via clippers). Note: clipping the hair from the biopsy site prevents hair from getting into the incision during the procedure and during closing, and hair removal allows for better contact between the tape closures and the skin (see 3.4).
- Have the operator sterilize the area with swabs pre-soaked with a topical antiseptic, (such as povidone-iodine or chlorhexidine gluconate for subjects allergic to iodine/shellfish). Begin in the center and work in concentric circles towards the outer edge of the clipped area. At a minimum, repeat twice more with a new pre-soaked swab each time.
2. Biopsy Procedure
- Have the operator remove disposable gloves, wash hands with soap and warm water, and don sterile surgical gloves using aseptic technique.
- Have technician #1 present the sterile fenestrated drape to the operator. Have the operator, using aseptic technique, place the drape over the biopsy site to maintain a sterile field.
- Have technician #1 present the operator a 5 ml syringe fitted with a 21 G needle while maintaining aseptic technique. Clean the top of the lidocaine vial with an alcohol swab.
- Have the operator immediately withdraw 5 ml of lidocaine. Remove the 21 G needle from the syringe and discard the needle into a sharps container.
- Have technician #1 present the operator with a 1-½ inch 25 G needle while maintaining aseptic technique. Have the operator place the 1-½ inch needle onto the syringe and evacuate the air bubbles from the syringe.
- Have technician #1 spray ethyl chloride on the incision site (~0.5 cm above the indelible ink mark on the skin) until the skin appears to “blanch.”
- Have the operator insert the needle approximately horizontal to the skin into the dermis, aspirate the needle, and then infiltrate with ~100 µl of lidocaine to produce a “bleb” 2-4 mm in diameter.
- Have the operator aspirate the needle (slightly withdraw the plunger of the syringe) to confirm that the needle has not been placed in a blood vessel. If blood appears in the syringe, withdraw the needle, discard in a sharps container, and begin again at 2.3.
- Have the operator advance the needle into the subcutaneous tissue, aspirate the needle, and then infiltrate the tissue with ~1 ml of lidocaine to form a bleb. Once the bleb has subsided, insert the 1-½ inch needle on the lidocaine-loaded syringe vertically into the incision site, stopping superficial to the fascia. Note: The subject may feel a slight momentary stinging sensation upon the initial injection of lidocaine (similar to a bee sting).
- Ensure that the operator does not infiltrate the muscle with lidocoine because it is myotoxic17-19.
- Have the operator aspirate the needle and then slowly inject the remaining 4 ml of lidocaine while withdrawing the needle from the thigh. Place sterile gauze over injection site and allow the subject to relax while the local anesthetic takes effect.
- Have the operator insert the needle approximately horizontal to the skin into the dermis, aspirate the needle, and then infiltrate with ~100 µl of lidocaine to produce a “bleb” 2-4 mm in diameter.
- After 2-3 min, have technician #1 present the operator a scalpel while maintaining aseptic technique.
- Have the operator lightly probe the biopsy site with the tip of the scalpel to confirm that the area is anesthetized. If necessary, inject another 3-4 ml of lidocaine into the incision site, see 2.4.1.2.
- Have the operator make a straight 1-cm incision through the skin and subcutaneous tissues (~2-3 mm above the ink mark) parallel to the femur.
- Have the operator insert the scalpel deeper to make an incision through the fascia into the muscle. Do this once in each direction. Note: The subject may feel a twinge or pressure with the deeper cut if the scalpel blade cuts into the muscle.
- Have technician #2 engage the subject in conversation and massage the opposite leg.
- Have the operator place a liberal amount of sterile gauze over the incision and biopsy site and apply direct pressure to the incision to reduce bleeding.
- Have technician #1 connect the 3-way metal stopcock to the disposable 60 ml syringe and the 30 cm extension tubing (Figure 1).
- Have technician #1 connect one end of the tapered plastic tubing connecter into the free end of the extension tubing and firmly insert the other end of the tapered plastic tubing connecter into the large end of a 200 µl pipette tip with ~15-18 mm of the tip cut off.
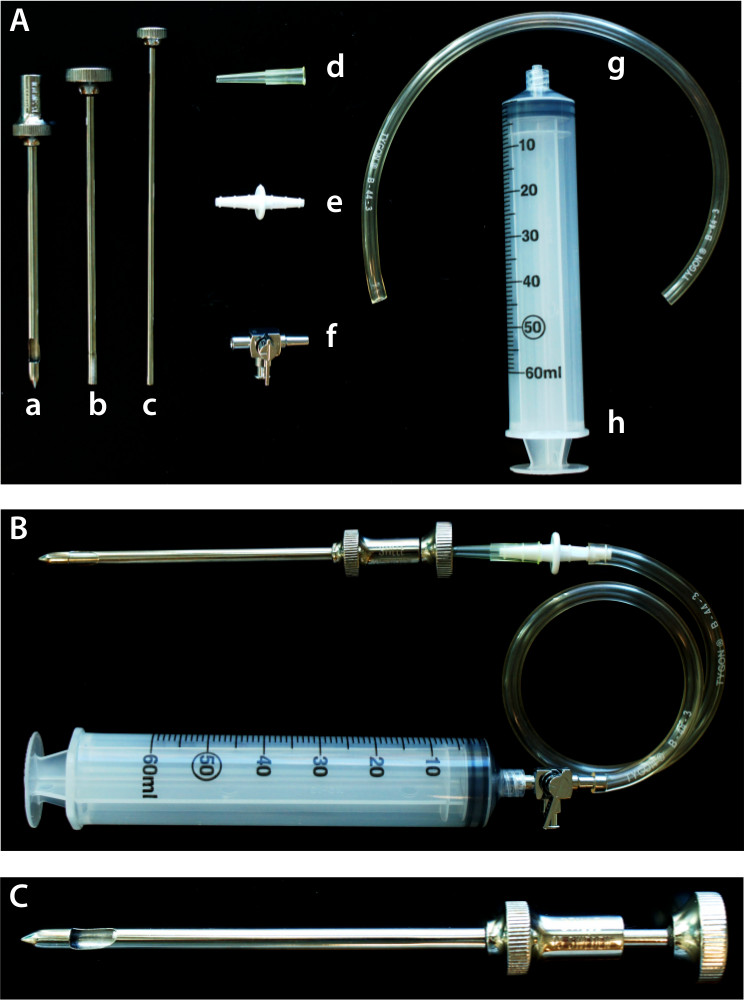
Figure 1. The Bergström needle. (A) The Bergström needle (5 mm) is composed of the (a) outer cannula and (b) inner trocar, the associated components include (c) plunger, (d) 200 µl pipette tip with ~15-18 mm cut off, (e) tapered plastic connector, (f) 3-way metal stopcock, (g) 30 cm extension tubing, and (h) disposable 60 ml syringe. (B) The Bergström needle (5 mm) and associated components assembled. (C) The inner trocar of the Bergström needle (5 mm) withdrawn approximately 1 cm opens the window of the outer cannula.
- After the bleeding has subsided, have technician #1 open the sterilized autoclave pouch and present the 5 mm biopsy needle and inner trocar (Figure 1) to the operator while maintaining aseptic technique.
- Have the operator assemble the needle (outer cannula and inner trocar), check alignment and sliding action.
- Have the operator firmly hold the needle assembly (outer cannula and inner trocar) with both hands to prevent the inner trocar from rotating. Have technician #1 firmly insert the cut pipette tip into the top of the inner trocar portion of the biopsy needle with a slight downward twisting motion. Ensure that technician #1 does not touch the operator or the biopsy needle, only the pipette tip.
- Have the operator introduce the biopsy needle into the tissue through the incision. Locate the incision in the fascia (an acquired “feel”) with the tip of the biopsy needle. Advance the needle just past the fascia and then angle the needle downward toward the floor as the needle is advanced into the muscle. Note: Subjects may experience some mild discomfort (e.g., “deep pressure,” or mild cramping sensation) as the incision through the fascia is located with the tip of the biopsy needle and the needle is advanced into the muscle.
- Have technician #2 instruct the subject to stay “relaxed” and not to contract their thigh muscles while the operator is advancing the needle into the muscle.
- Once the biopsy needle is in position, have the operator signal technician #1 to open the disposable 60 ml syringe.
- Have technician #1 rapidly pull the disposable 60 ml syringe open to the 40-50 cc mark to create suction within the biopsy needle.
- Have the operator pull the inner trocar out approximately 1 cm to open the window of the outer cannula while maintaining the position of the outer trocar within the muscle. Have the operator rapidly close the inner trocar to cut (clip) and collect the muscle sample. Have the operator signal technician #1 to release suction.
- Have technician #1 open the stopcock to the room to release the suction.
- Have the operator rotate the biopsy needle 90° and repeat the process. If required, have the operator repeat the rotation procedure up to 3x (for a total of 4 clips).
- Have the operator apply direct counter-pressure to the incision site with sterile gauze while removing the biopsy needle from the thigh, being careful not to catch fascia or skin. If significant resistance is felt, re-cut while applying a twisting motion to the inner trocar.
- Upon removal of the biopsy needle from the thigh, have the operator pull the inner trocar back 1 cm to visually inspect the lumen of the outer cannula to estimate if an adequate amount of tissue was collected.
- Have the operator hand the biopsy needle to technician #1. To maintain aseptic technique ensure that technician #1 only touches the needle, not the operator. Have technician #1 hand the biopsy needle to technician #3.
- Have technician #3 remove the tissue from the biopsy needle.
- Have technician #3 use the plunger (Figure 1) and a pair of fine tip forceps to ensure that all muscle tissue is removed from the inner trocar and outer cannula.
- Have technician #3 quickly weigh the sample to confirm that an adequate amount of muscle tissue was collected and place the samples on an ice-cold dissection block.
- Have technician #3 carefully dissect visible connective tissue and fat from the muscle samples. Have technician #3 prepare the muscle samples for storage according to downstream analyses. For example, immediately place samples in a cryovial and snap freeze in liquid nitrogen, mount and freeze for histology, or place in a cryovial with RNase inhibitor, etc.
- If necessary, repeat the procedure with a second sterilized biopsy needle while maintaining aseptic technique.
3. Closure
- Have the operator apply direct pressure to biopsy site with sterile gauze and an ice pack for 10-15 min.
- Once hemostasis is achieved, have the operator use alcohol prep pads to remove dried blood from the area around the incision.
- Have technician #1 present a tube of topical surgical adhesive and applicator to the operator. Have the operator assemble the tube of surgical adhesive and applicator without touching the applicator tip or the top of the tube.
- Have the operator pull the incision closed with one hand while applying a single layer of surgical adhesive over the top of the dry incision with the other hand. After the adhesive cures (~ 90 sec), apply tape closuresperpendicular to the incision. Alternatively, close the incision with two sterile 4-0 sutures.
- Have the operator apply direct pressure by placing 3-4 2” x 2” non-sterile gauze pads on the incision site and secure with self-adhering adhesive wrap.
- Have the operator provide the subject verbal and written instructions on proper wound care, normal and abnormal reactions, and activity guidelines for the following 1 to 4 days (see online supplement 2).
The muscle biopsy procedure as described above allows the researcher to quickly and consistently collect skeletal muscle tissue samples. The typical yield in healthy, athletic subjects is 200 mg or more in a single pass with 3-4 clips. The procedure takes 15-20 min, most of which is spent in preparation for the incision. In exercise-based studies, muscle samples are often taken pre- and post-exercise, with one or two samples collected during recovery. With this design, the hair on the post-exercise (contralateral) thigh is clipped and the incision site is pre-marked with a fine point permanent marker while the pre-exercise thigh is being prepared for the procedure. Doing so allows the muscle biopsy to be taken in 8-10 min during20 or after a bout of prolonged exercise. Alternatively, when investigating shorter periods of exercise (e.g., 30 min or less) an incision(s) can be made prior to exercise, covered with sterile dressing and fastened with surgical tape, thus, allowing the biopsy sample to be taken rapidly (10 sec21 to 4 min22) after completing a bout of exercise. The relative quickness of the procedure enables the researcher to capture cellular and molecular events before, during, and after a bout of exercise, and to test the interaction effect of a nutritional intervention.
The ASU Human Performance Laboratory has published several sports nutrition based papers utilizing data from muscle tissue biopsy samples. Important scientific discoveries made from the ASU research group include:
Gene expression of IL-1β, IL-6, IL-8, and TNF-α is increased in skeletal muscle tissue obtained from experienced endurance athletes after 3 hr of running. Carbohydrate intake (60 grams/hr) attenuated IL-6 and IL-8 mRNA levels despite having no effect on skeletal muscle glycogen depletion8 (Figure 2).
A 2-hr intensive resistance training bout increased muscle tissue cytokine mRNA for IL-1β, IL-6, IL-8, and TNF-α in 30 experienced weight lifters (i.e., same cytokines as elevated following running). The increases in muscle tissue mRNA expression were large but without corresponding increases in plasma cytokine levels. Carbohydrate intake did not influence the pattern of change in muscle tissue cytokine mRNA expression9.
Carbohydrate ingestion by 15 trained cyclists attenuated plasma IL-6 compared to placebo, but had no influence on muscle tissue glycogen depletion or IL-6, IL-8, TNF-α mRNA expression following 2.5 hr of cycling11.
Quercetin (1,000 mg/day for 3 weeks) ingestion by 40 trained cyclists did not alter exercise-induced increases in muscle tissue NF-κB, COX-2, IL-1β, IL-6, IL-8, or TNF-α mRNA expression compared with placebo15.
In contrast to what was found in mice23, 1,000 mg/day quercetin for 2 weeks had modest, but insignificant, effects on markers of mitochondrial biogenesis in 26 untrained human subjects13.
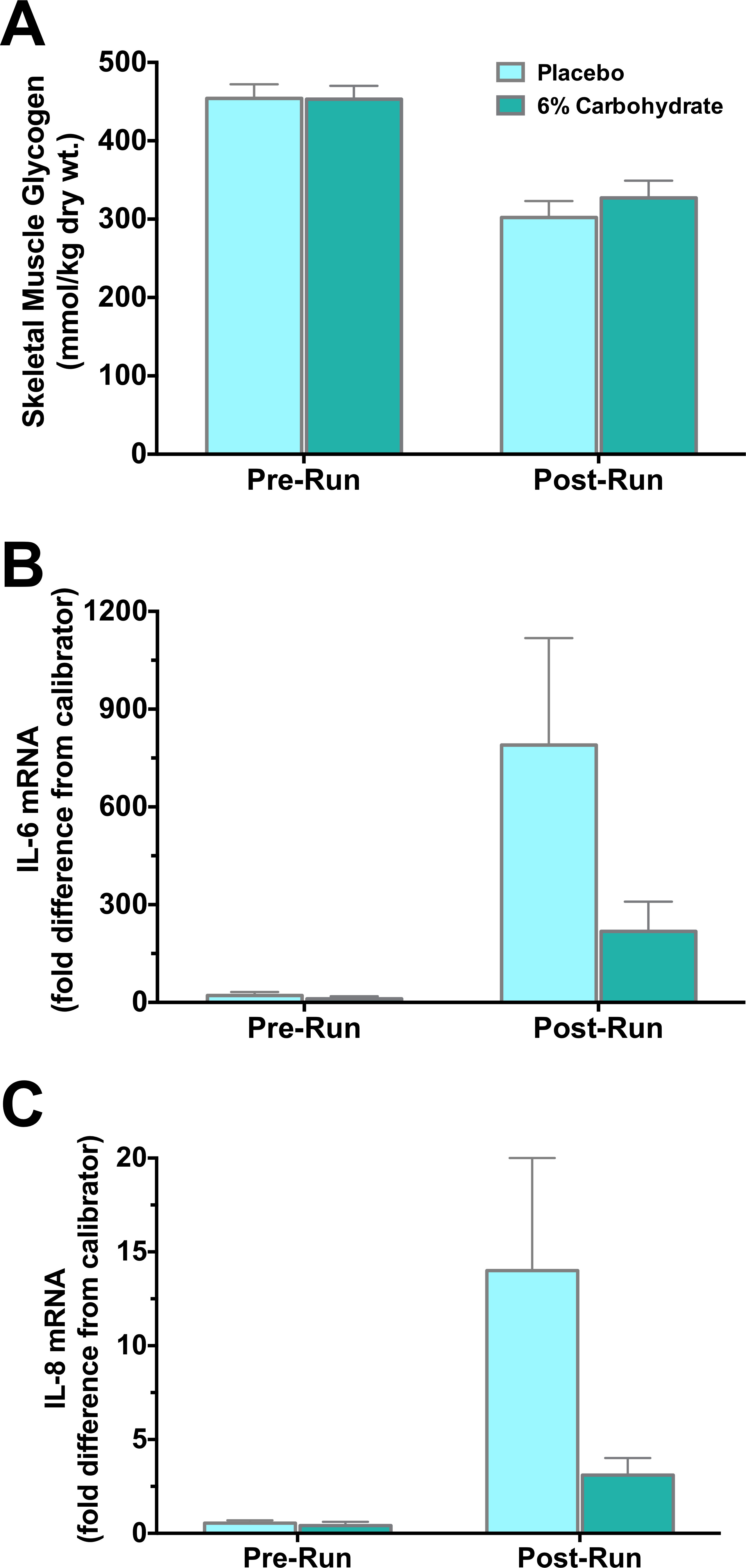
Figure 2. Data obtained from human skeletal muscle tissue biopsies. In a randomized, placebo controlled, crossover study male endurance athletes (n = 16) ran on treadmills for 3 hr at 70% VO2max and consumed a 6% carbohydrate beverage or a placebo beverage at a rate of 1 L/hr8. Skeletal muscle tissue biopsies were taken pre- and post-exercise, immediately placed on an ice-cold dissection block, and visible connective tissue and fat was carefully removed. The biopsy sample was then placed in a cryovial, frozen in liquid nitrogen, and stored at -80 °C until analysis. (A) Carbohydrate ingestion did not influence skeletal muscle glycogen depletion (p = 0.246, interaction effect). However, carbohydrate ingestion tended to attenuate the increase in (B) skeletal muscle tissue interleukin (IL)-6 mRNA levels, and (C) skeletal muscle tissue IL-8 mRNA levels (p = 0.071 and p = 0.063, interaction effect, respectively)8.
| Item | Quantity per biopsy |
| Gloves, non-sterile | 3 |
| Durasorb blue pad | 2 |
| Face mask | 1 |
| Prep razor, disposable | 1 |
| Shave cream | partial can |
| Permanent marker / indelible marker | reusable |
| Betadine Swabsticks (3 pack) | 1 |
| Sterile surgical gloves (size dependent) | 1 |
| Fenestrated towel drape | 1 |
| Ethyl chloride spray | 0.1 |
| Lidocaine (1% w/o Epi) | 5 cc |
| 5 ml syringe w/ 21 G needle | 1 |
| 25 G 5/8" needle | 1 |
| 25 G 1 1/2" needle | 1 |
| Single-use scalpels w/ #11 blade | 1 |
| Sterile 4 x 4 gauze pads | 4 |
| Packaged sterilized Bergström biopsy needle | 1 |
| 60 ml Syringe | 1 |
| Extension tubing | ~75 cm |
| Metal stopcock | 1 |
| Plastic connector | 1 |
| Cut yellow (1-200 μl) pipette tip | 1 |
| Alcohol swabs | 5-10 |
| Octylseal, liquid sutures | 1 |
| Steri-strip 1/2" x 4" | 1 |
| Bandage | 1 |
| Non-sterile 2 x 2 (or 4 x 4) gauze pads | 2 (or 1) |
| Adhesive bandage (5 m roll) | 0.25 |
| Paper tape to secure adhesive bandage | ~30 cm |
Table 1. Muscle Biopsy Materials List.
